
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-033
CHIP - Choice OR Only Option..!! For Complicated Post Covid Case With Severely Calcified LM Trifurcation Lesion
By Harsimran Singh, Nagendra Boopathy Senguttuvan, Ramesh Sankaran, Vinod Kumar Balakrishnan, S Sadhanandham, Venkata Balasubramaniyan Jayanty, Preetam Krishnamurthy, Manokar Panchanatham, Thoddi Ramamurthy Muralidharan
Presenter
Harsimran Singh
Authors
Harsimran Singh1, Nagendra Boopathy Senguttuvan2, Ramesh Sankaran2, Vinod Kumar Balakrishnan2, S Sadhanandham2, Venkata Balasubramaniyan Jayanty2, Preetam Krishnamurthy2, Manokar Panchanatham2, Thoddi Ramamurthy Muralidharan2
Affiliation
Pancham Hospital, India1, Sri Ramachandra Institute of Higher Education and Research, India2,
View Study Report
TCTAP C-033
CORONARY - Bifurcation/Left Main Diseases and Intervention
CHIP - Choice OR Only Option..!! For Complicated Post Covid Case With Severely Calcified LM Trifurcation Lesion
Harsimran Singh1, Nagendra Boopathy Senguttuvan2, Ramesh Sankaran2, Vinod Kumar Balakrishnan2, S Sadhanandham2, Venkata Balasubramaniyan Jayanty2, Preetam Krishnamurthy2, Manokar Panchanatham2, Thoddi Ramamurthy Muralidharan2
Pancham Hospital, India1, Sri Ramachandra Institute of Higher Education and Research, India2,
Clinical Information
Patient initials or Identifier Number
2751019
Relevant Clinical History and Physical Exam
A79 yr old male admitted with fever and cough in desaturated state. Hewas diagnosed with covid-19 (RT-PCR +),and was managed conservatively as per standard protocol. He developed acutepulmonary edema after 14 days of his illness. Developedhypotension and was started on inotropes. Diagnosed with evolved AWMI (KILIPS class III on mechanical ventilator). Repeat covid 19 test was negative.Known- DM II , Hypertension, AKIBP- 100/70mmHg (on support) HR-100/MinuteCVS- S1S2S3+RS- B/L crepitation +
Relevant Test Results Prior to Catheterization
ECG- Q wave in V2-V5 with ST Elevation2D TTE- Severe LV dysfunction (EF-30%) with grade I diastolic dysfunction. Severely hypokinetic LAD territory.Trop I- 8.9 ng/mlNTproBNP- 8110 pg/mlHb - 10.8 gm/dlTC- 11200 cells/mcLPlatelets- 2.5 lakhsBUN- 64 mg/dlCreatinine- 1.3 mg/dlCT Thorax- B/L moderate pleural effusion (right>left) with minimal consolidation on right side.
Relevant Catheterization Findings
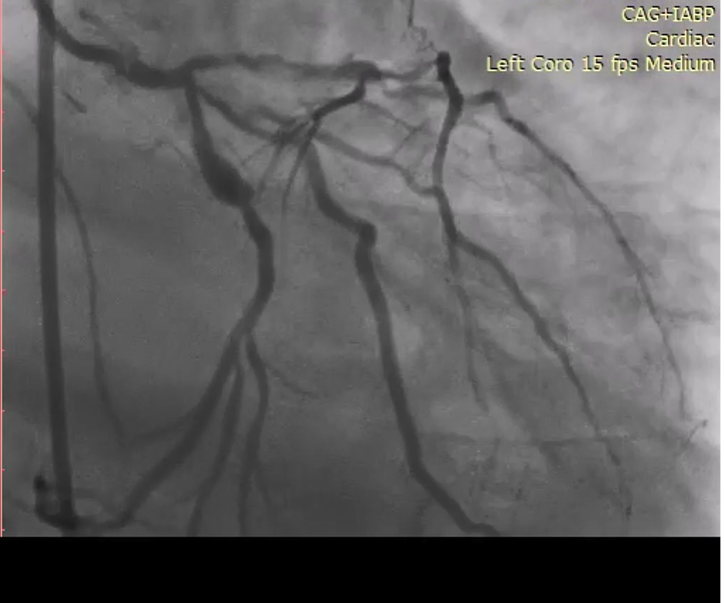
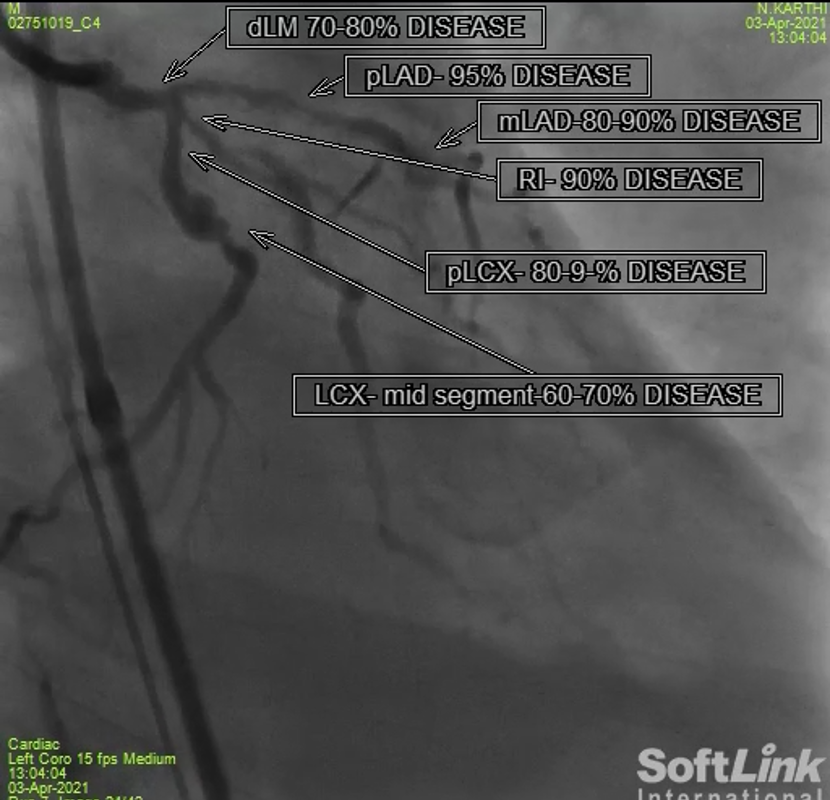
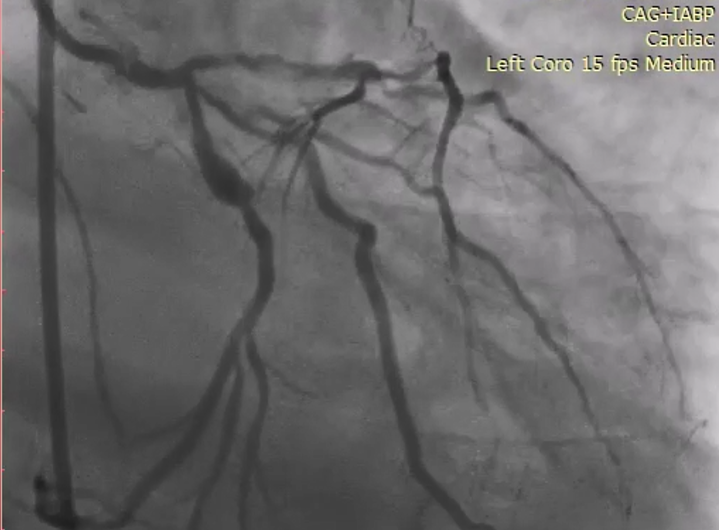
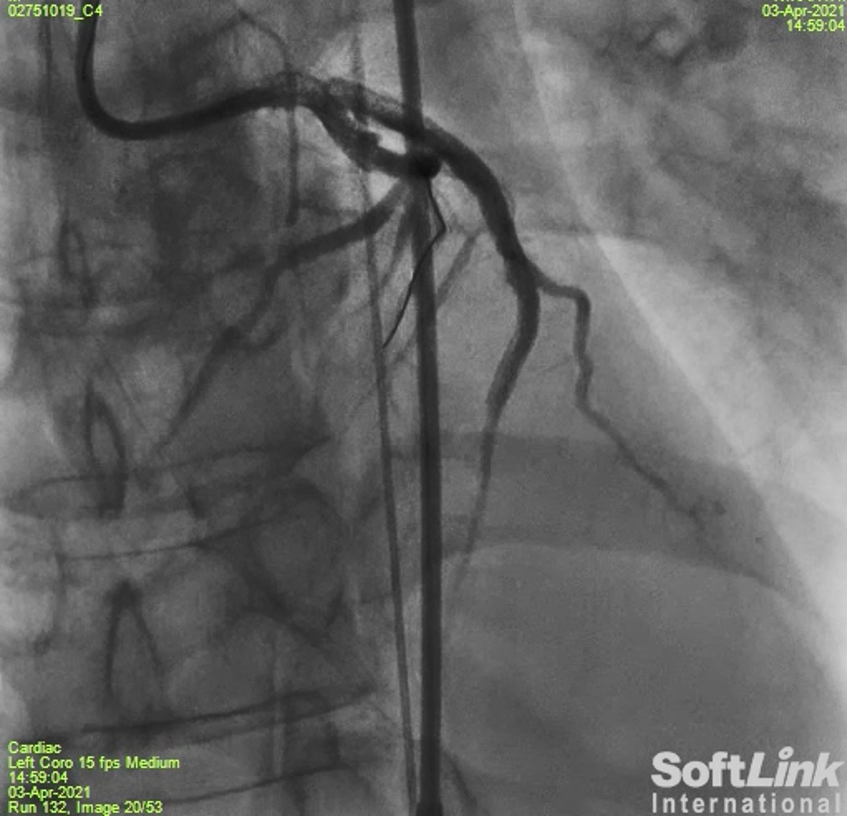
Coronary Angiogram - Denselycalcified - Distal LM had 50-60% stenosis. LAD had long segment lesion extending fromostial to mid segment with maximum severity of 90-95%. Ramus intermedius has ostial 90% lesion.LCX was a dominant vessel with 80-90% ostial lesion. RCA has 70-80% ostioproximallesion.

 Media25.avi
Media25.avi
Media26.avi
Media27.avi
Interventional Management
Procedural Step
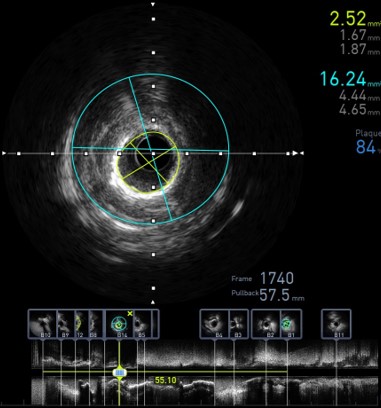
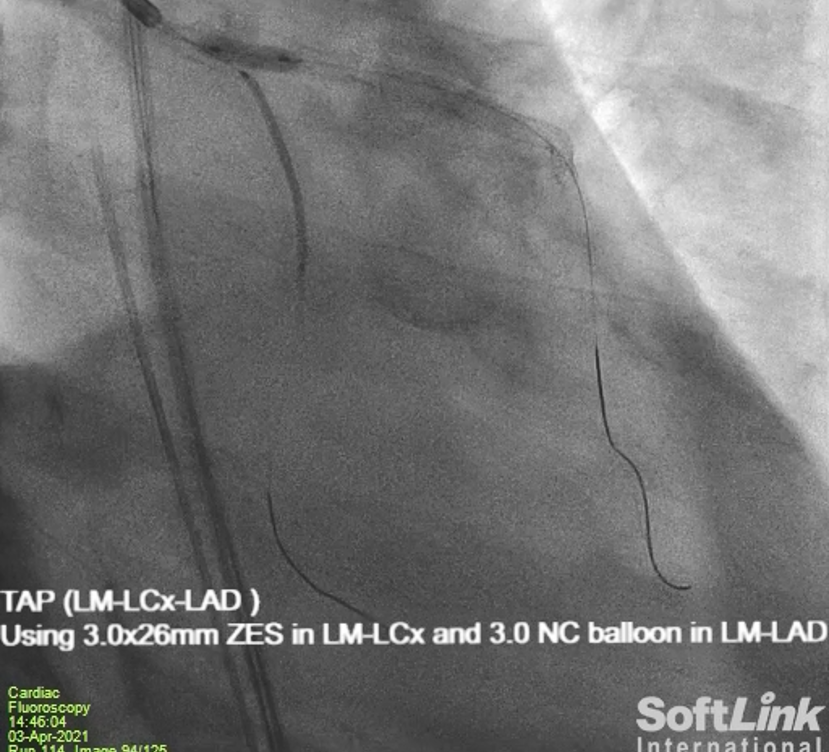
-Lt. femoral artery cannulated with 7F long sheath-IABP placed through rt. femoral artery-TPI through RT. femoral vein-With 7F 3.5 EBU (Terumo, Japan) guiding Lt. coronary artery hooked-Using fine cross microcatheter (Terumo, Japan) runthrough wire (Terumo,Japan) exchanged with grand slam wire (Asahi,Japan)-Predilatation in LAD using 1.5x10 mm ryurei balloon (Terumo, Japan) f/b 2x10 mm apollo balloon (Brosmed, China)-IVUS done-I/V/O densely calcified vessel predilation with 2.5x10 mm accuforce (Terumo,Japan) balloon followed by IVL with shockwave C2 3X12 mm balloon (Shockwave medical, USA)-Prepare LCX with 2x10 mm ryurei balloon (Terumo,Japan) f/b 3x10 mm OPN balloon (sismedical, Switzerland)-LAD stented with 2.75x30 mm Resolute DES (Medtronic, USA) and 3.5x38 mm Resolute DES-Ostial flarring done with same stent balloon using modified Tzabo wire technique (Terumo,Japan)-POT to LM done using 4.5x6 mm Accuforce balloon (Terumo, Japan)-BMW (Abbot, USA) wire recrossed in LCX-POBA to RI done using 2.5x15 mm Tazuna balloon (Terumo, Japan)-LCX predilated with 2.5x 12 mm accuforce balloon ((Terumo,Japan)-LAD post dilated with 3x10 mm apollo balloon (Brosmed,China). Same balloon placed in LM to LAD area and 3x26 mm resolute DES was kept in the ostial LCX with one strut protruding into LM (TAP technique)-IVUS run showed satisfactory results
Case Summary
-COVID-19 infection makes a stable plaque into unstable plaque.
-Severely calcified lesions associated with significant thrombus can be safely handled by lithotripsy
-Preparation of vessel bed is essential for better results