
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-009
Left Main Bifurcation PCI in a Patient With Non-ST- Elevation Acute Coronary Syndrome Complicated by Ventricular Tachycardia
By Dileep Kumar Tiwari, Amjad Ali
Presenter
Dileep Kumar Tiwari
Authors
Dileep Kumar Tiwari1, Amjad Ali2
Affiliation
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
View Study Report
TCTAP C-009
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Left Main Bifurcation PCI in a Patient With Non-ST- Elevation Acute Coronary Syndrome Complicated by Ventricular Tachycardia
Dileep Kumar Tiwari1, Amjad Ali2
Baderiya Metroprime Hospital, India1, Sagar Multispeciality Hospital, India2,
Clinical Information
Patient initials or Identifier Number
YD
Relevant Clinical History and Physical Exam
A seventy-two-year-old gentleman, who has long-standing hypertension andtype 2 diabetes mellitus, was rushed to the emergency room with complaints ofsudden onset chest discomfort, uneasiness, and perspiration for two hoursduration. He fell at home twice and got a lacerated wound over the scalp anddeveloped a large left supraorbital hematoma. In the emergency room, hewas throwing repeated episodes of ventricular tachycardia (VT) which werecardioverted with DC shock each time.
Relevant Test Results Prior to Catheterization
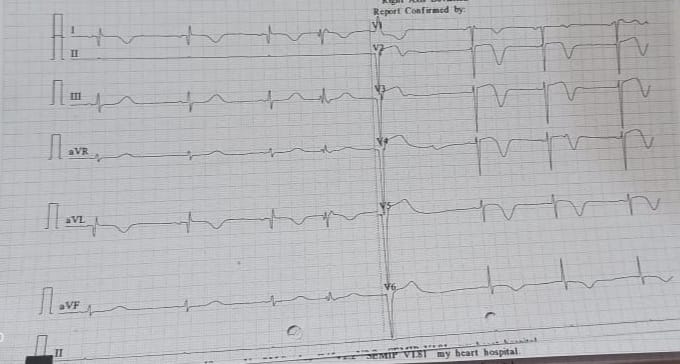
ECG was taken between the episodes of VT which revealed ST Coving and deep T inversion in lead I, aVL, and V1 - V6. A fusion beat was also seen. His blood pressure was 90/60 mmHg and hence put on inotropic support. The loading dose of Ticagrelor 180 mg, Aspirin 325 mg, and Atorvastatin 80 mg was given. Echocardiography showed global LV hypokinesia with akinetic LAD territory with preserved myocardial thickness. His LV ejection fraction was 28%
Relevant Catheterization Findings
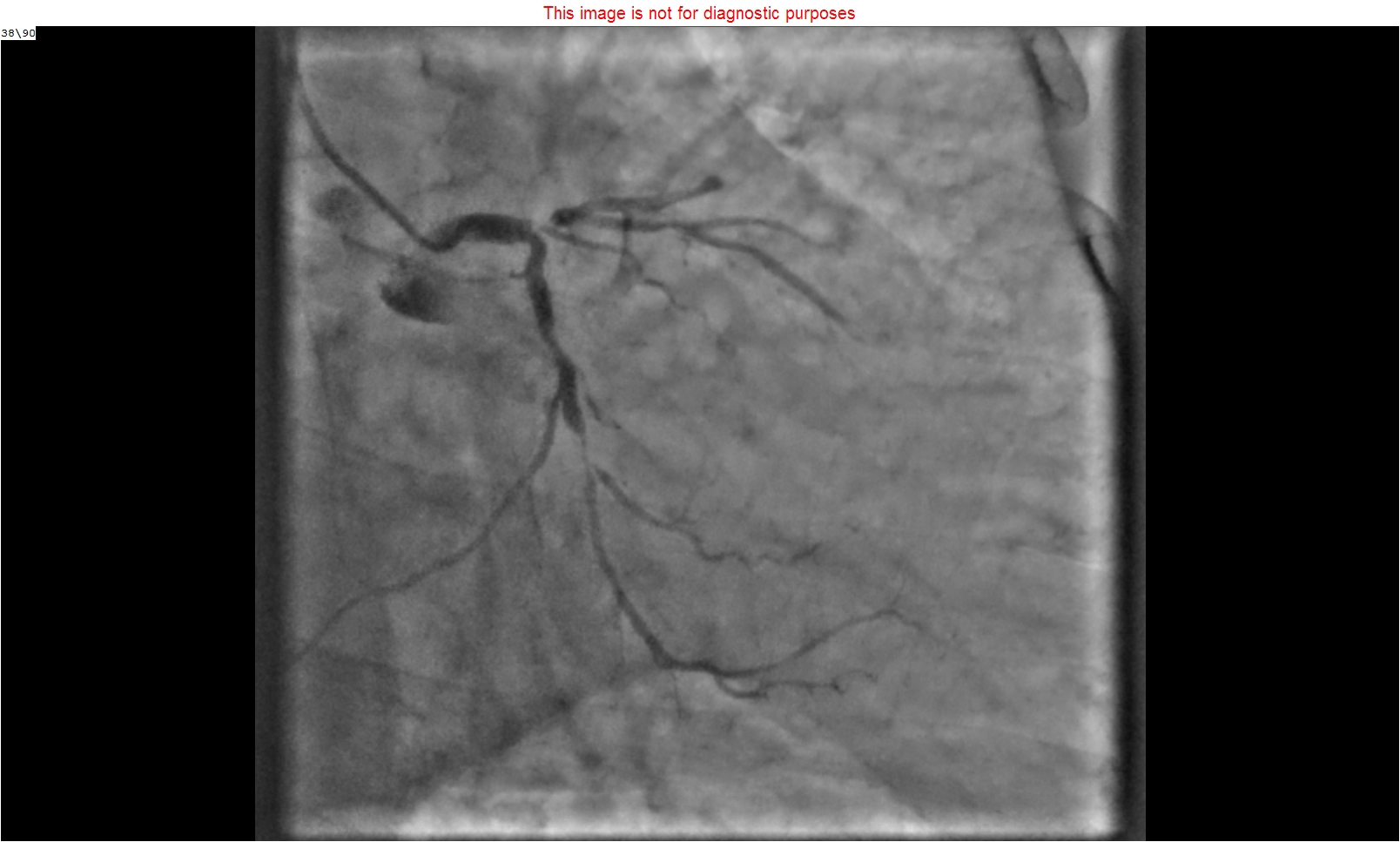
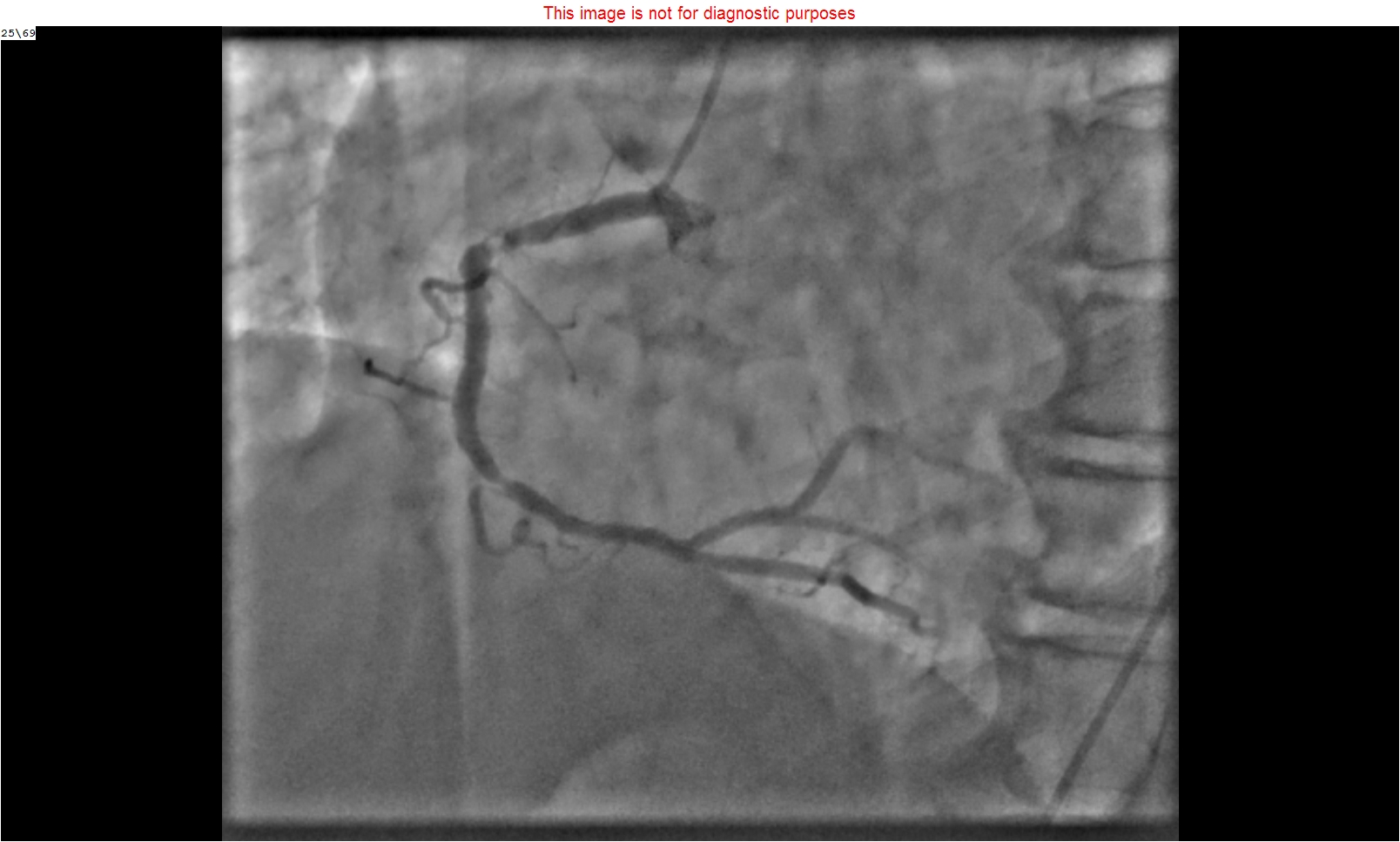
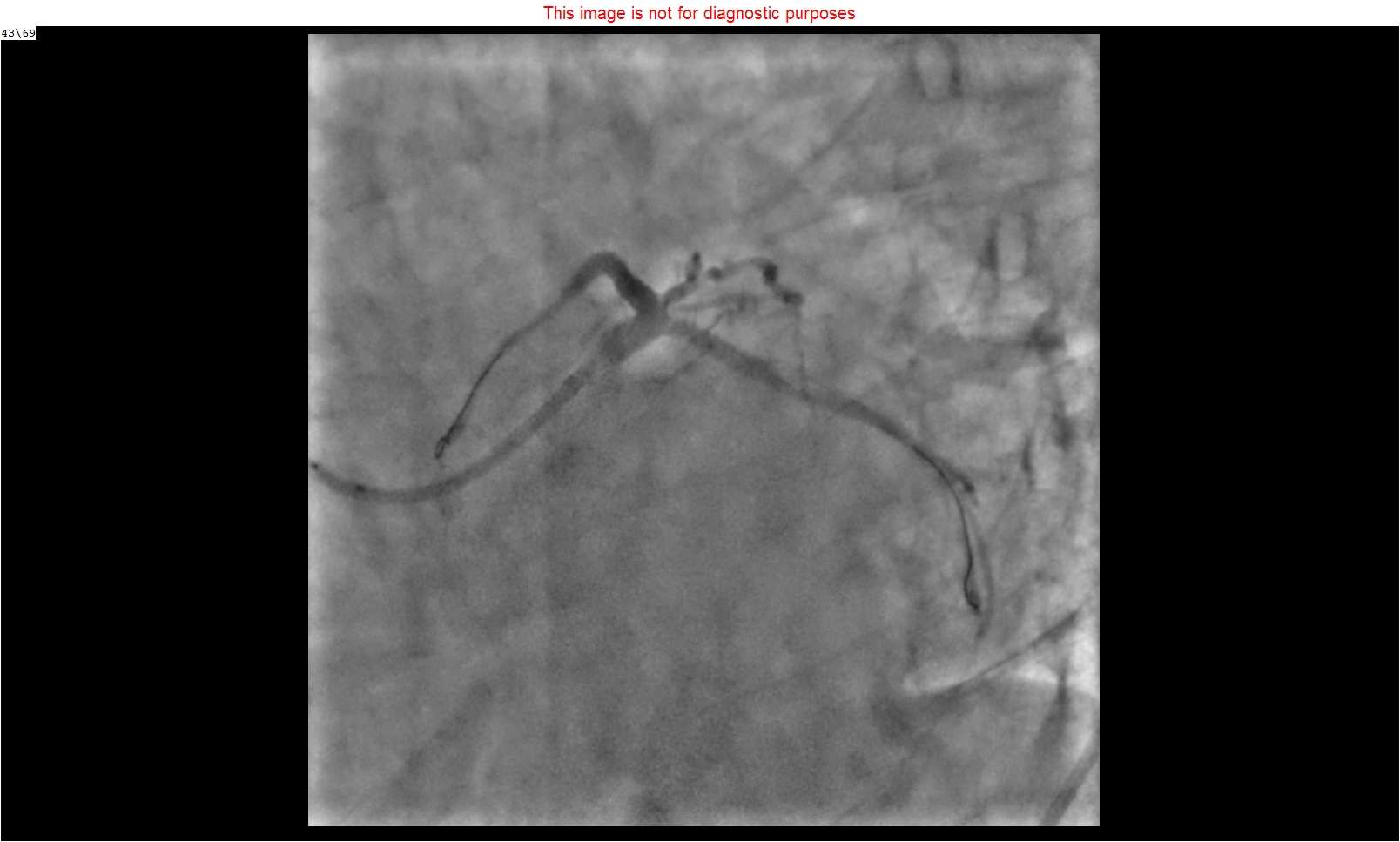
After taking written high-risk consent, the coronary angiogram was performed which revealed a thrombotic left main bifurcation lesion (Medina 1, 1, 1.) with distal left main (LM) 70-80%, ostial left anterior descending artery (LAD) 90-95% and ostial Left circumflex (LCx) had 70 % stenosis. There was hardly any flow to distal LAD. The right coronary artery (RCA) also had significant stenosis. During angiogram, the patient had multiple episodes of VT and had to be cardioverted each time.
Interventional Management
Procedural Step
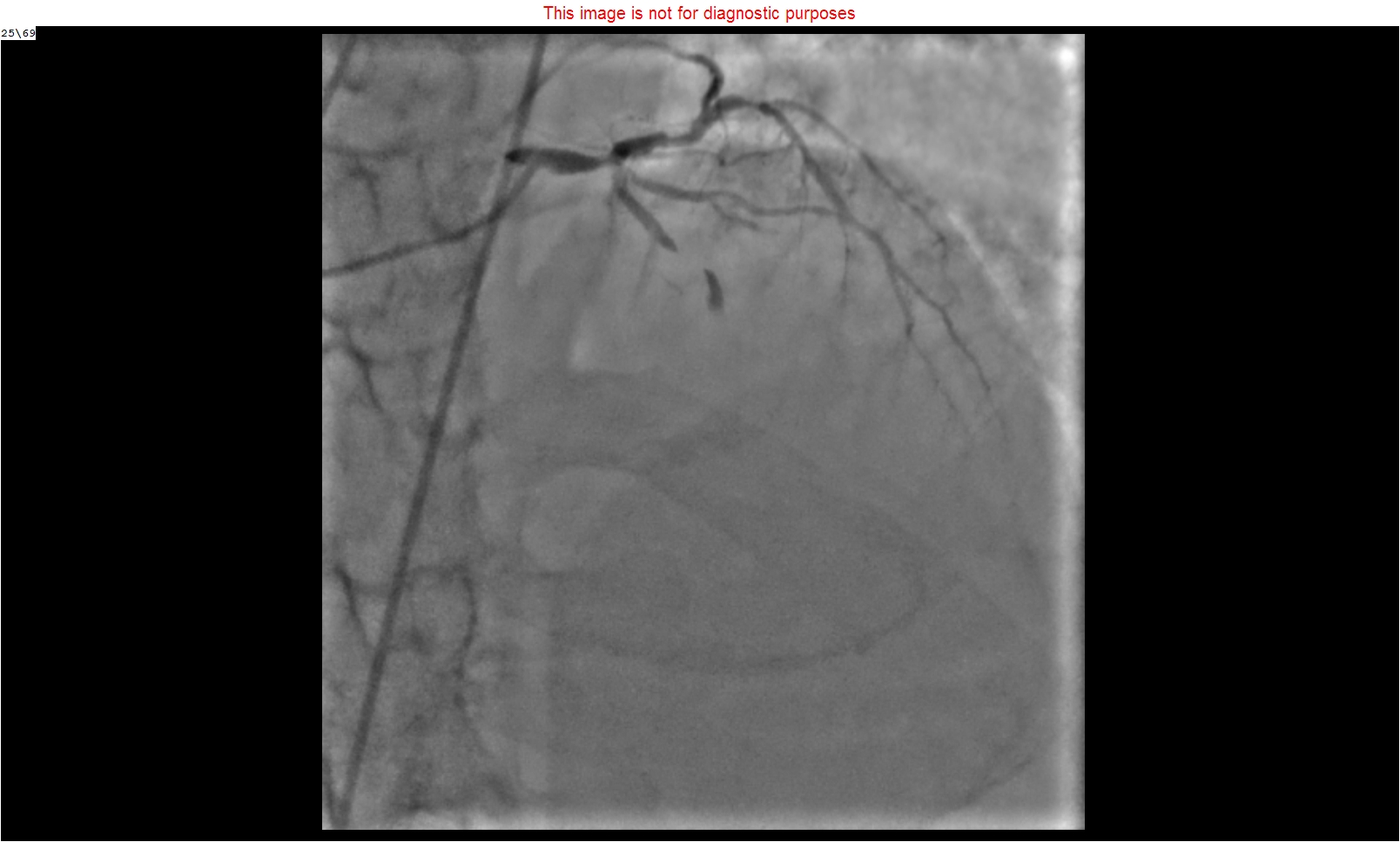
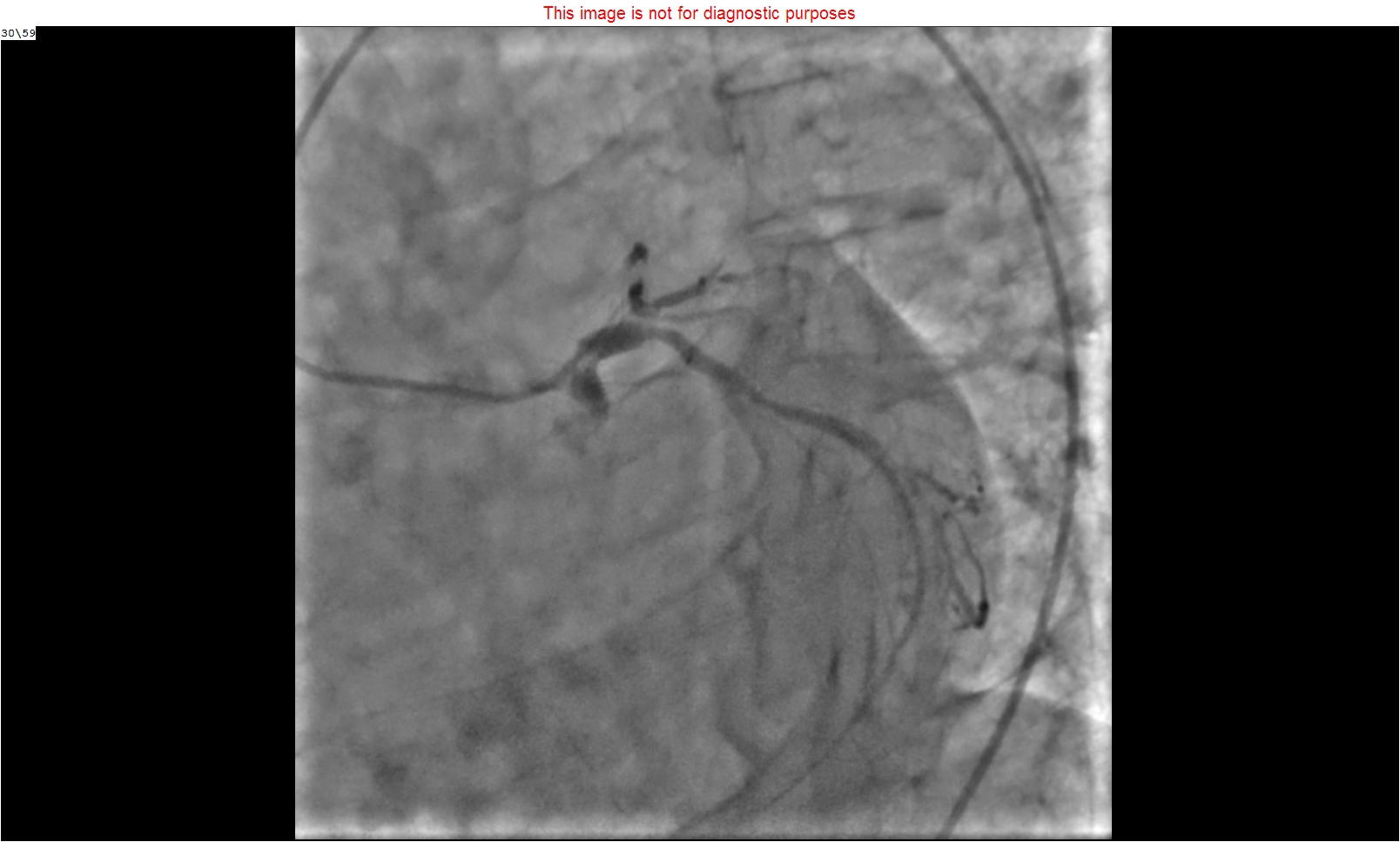
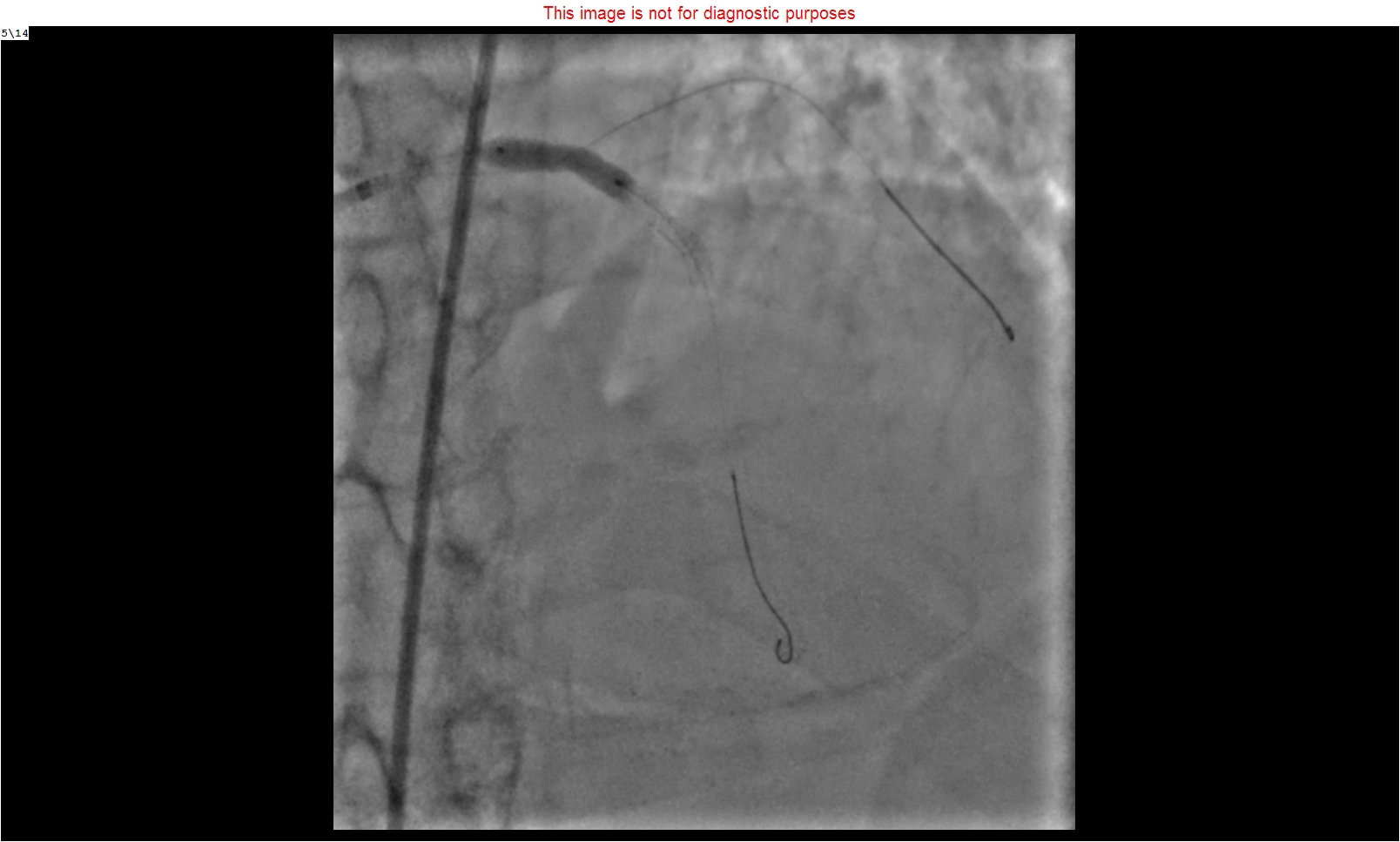
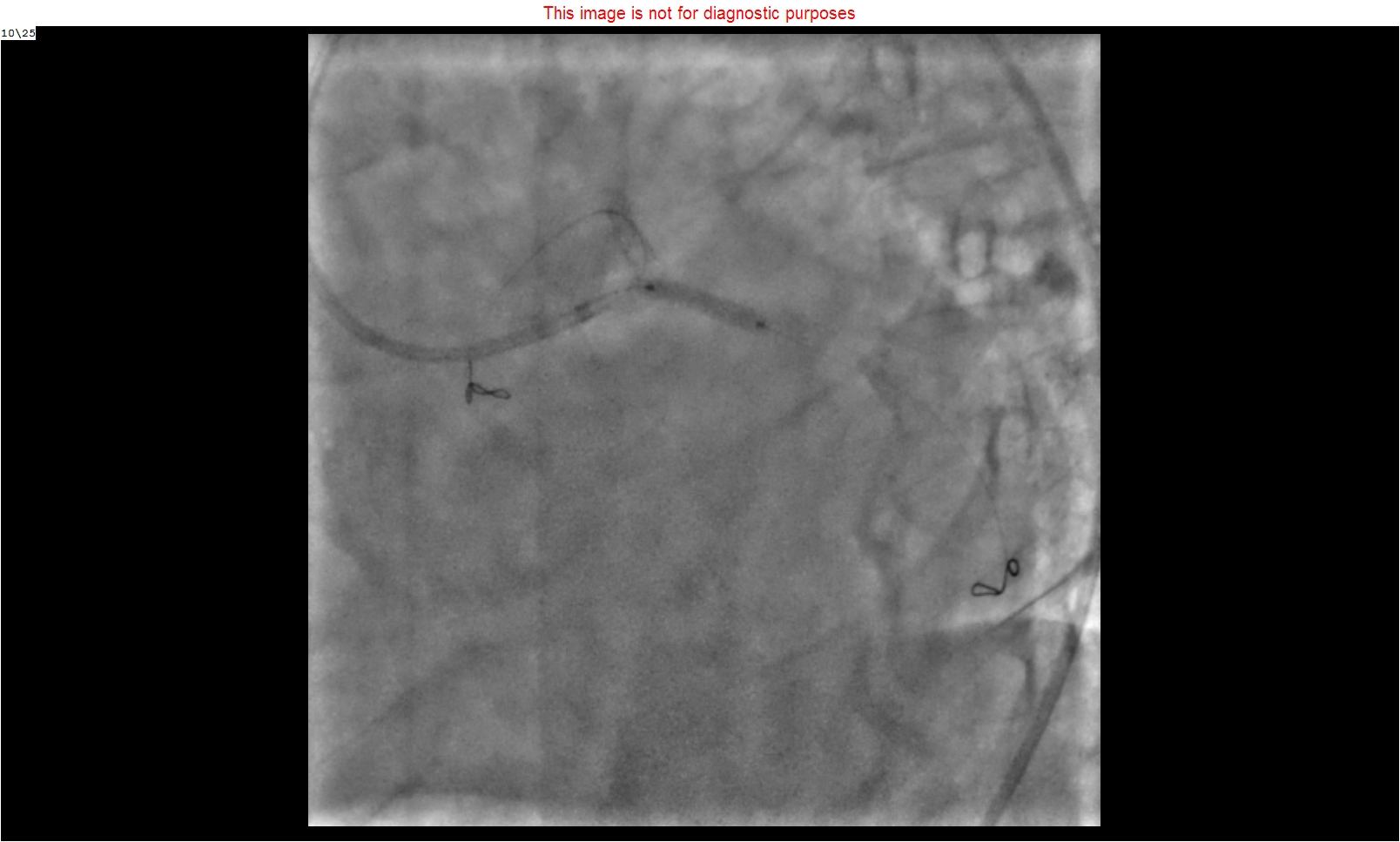
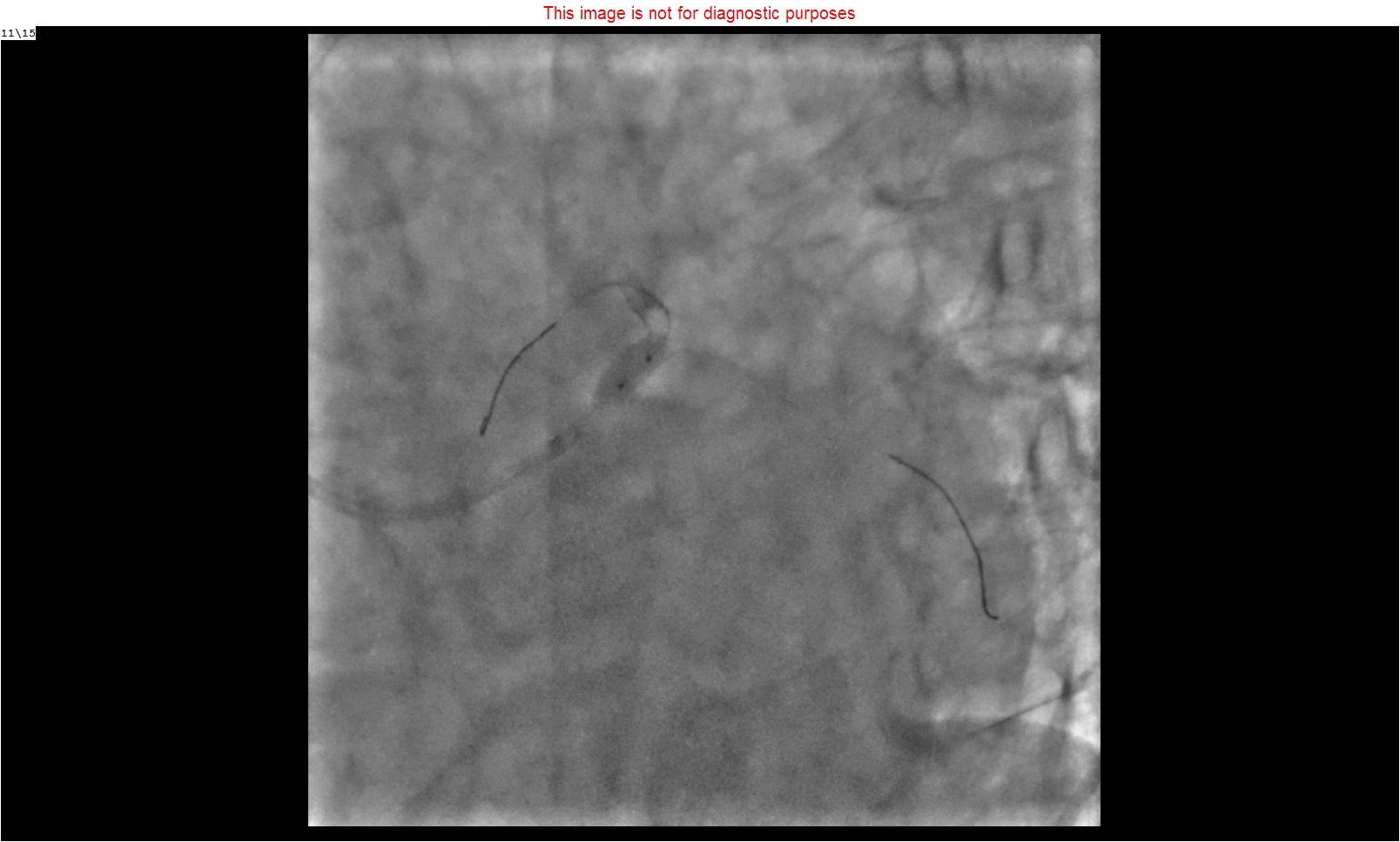
Our primary aim was to restore the blood flow as early as possible. Hence the PCI to left main bifurcation with intra-aortic balloon pump (IABP) support was planned. Because of some technical problem, there was a delay in the IABP to start, so we proceeded for PCI on inotropic support. The left main artery was hooked with an extra backup 3.5, 7 F' guiding catheter. Lesions were crossed with Hi-torque balanced middleweight (Abbott vascular) 0.014” wire in LAD and Rinato (Asahi intecc) 0.014" wire in LCx. LAD lesion was predilated with 2 x 12 mm semi-compliant (SC) balloon at 12 atm pressure. 3.5 x 23 mm Xience Xpedition (Abbott Vascular) stent deployed in mid LAD at 12 atm pressure and another 4.0 x 18 mm Xience Xpedition (Abbott Vascular) overlapping stent deployed from left main to LAD at 12 atm pressure. Post dilatation was done with 4.0 x 12 mm non-compliant (NC) balloon at higher pressures. LCx lesion was recrossed, and stent strut dilated sequentially with 1.5 x 10 mm and 2 x 12 mm SC balloon each at 12 atm pressures. Considering the favorable carinal angle, another 2.75 x 15 mm Xience Xpedition (Abbott Vascular) stent was deployed at 12 atm. pressure in LCx using the T stent technique. Final kissing balloon dilatation was done with 3.5 x 12 mm NC balloon in LAD and 2.75 x 12 mm NC balloon in LCx at 12 and 8 atm pressure respectively. The final POT was done with 4.5 x 8 mm NC balloon at 20 atm. The end result was good with distal TIMI 3 flow. No VT episodes occurred further.
Case Summary
In the case of VT due to an acute coronary syndrome, time is the life, and restoring the blood supply to jeopardized myocardium as early as possible by the opening of the culprit's vessel is the key to survival. In an emergency, left main bifurcation stenting should be done with a minimal time-taking technique if anatomy favors like in this case (T stenting technique). IABP could be considered but weigh the cost of time versus effectiveness.