
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-152
OCT Guided Ambiguous Lesion of NSTEMI Patient
By Fani Suslina Hasibuan, Achmad Fauzi Yahya
Presenter
Fani Suslina Hasibuan
Authors
Fani Suslina Hasibuan1, Achmad Fauzi Yahya2
Affiliation
RSUD Dr R Koesma, Indonesia1, Dr. Hasan Sadikin Central General Hospital, Indonesia2,
View Study Report
TCTAP C-152
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular
OCT Guided Ambiguous Lesion of NSTEMI Patient
Fani Suslina Hasibuan1, Achmad Fauzi Yahya2
RSUD Dr R Koesma, Indonesia1, Dr. Hasan Sadikin Central General Hospital, Indonesia2,
Clinical Information
Patient initials or Identifier Number
Mrs IK
Relevant Clinical History and Physical Exam
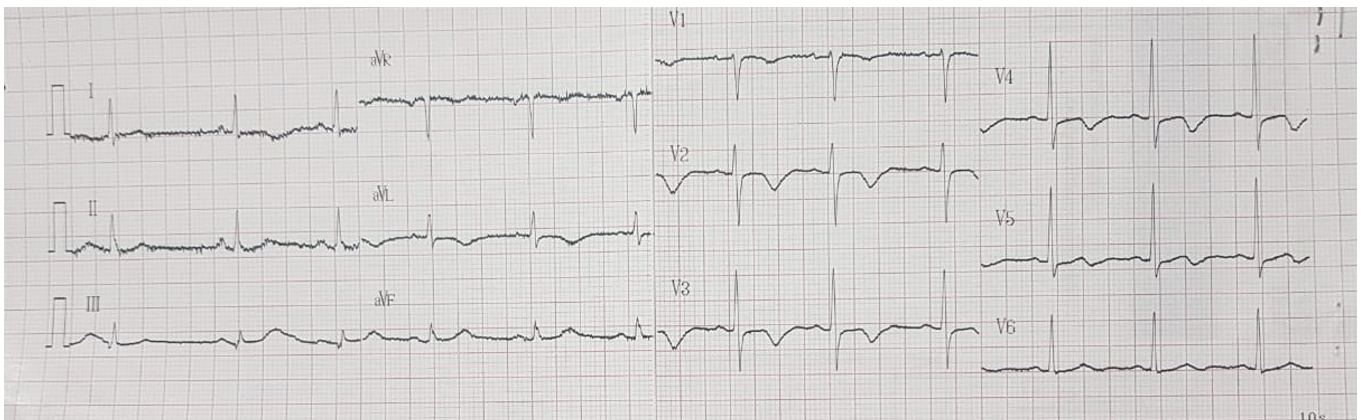
A 69 year-old female presented Non ST Elevation Myocardial Infarction came to our hospital. Cardiovascular risk factor was Hypertension.The ECG showed ST depression at anterior lead. Her physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
Troponin level was elevated . Echocardiography showed preserved LVEF.
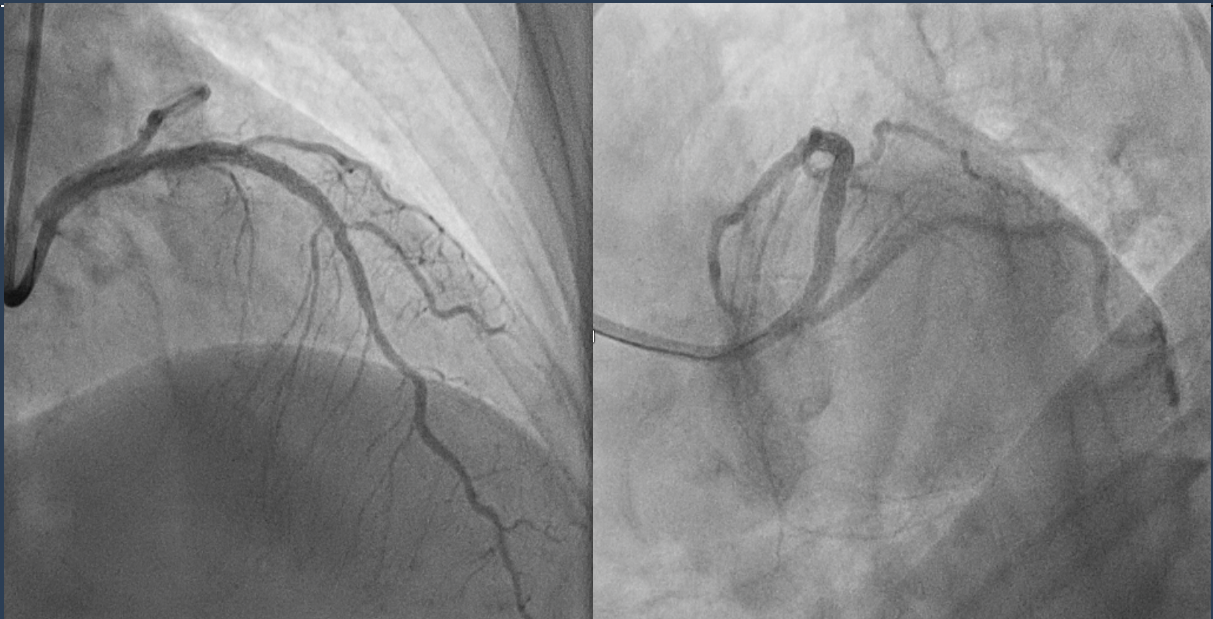
Relevant Catheterization Findings
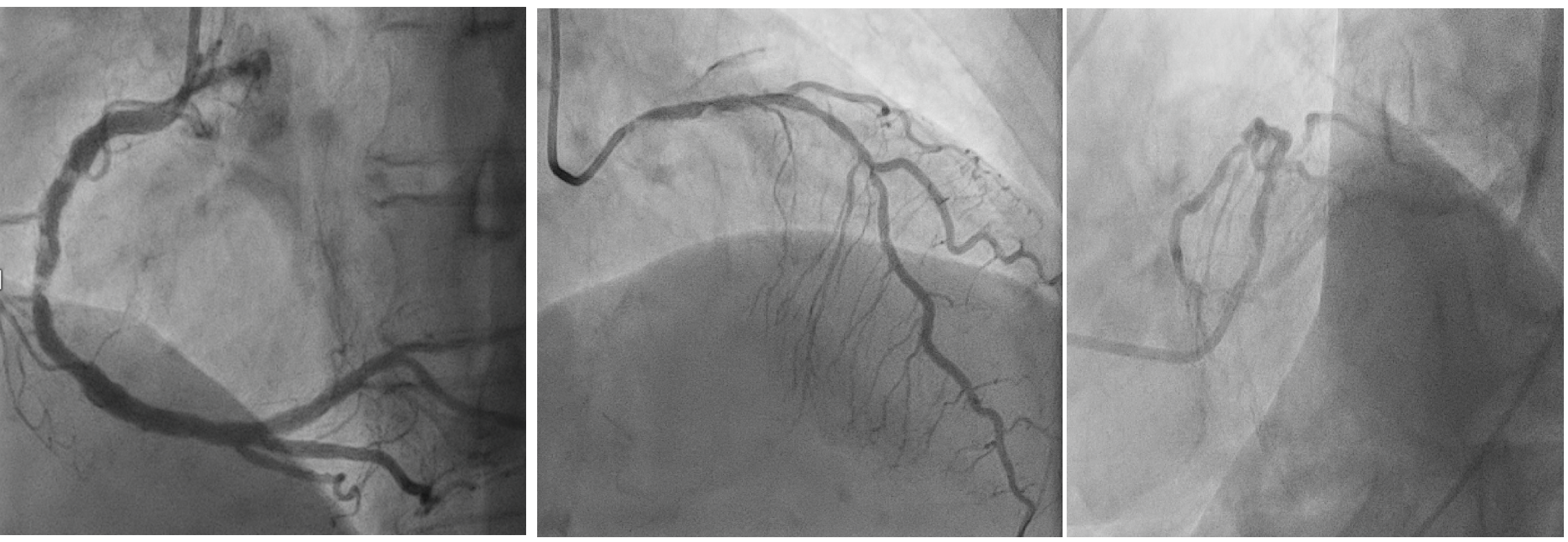
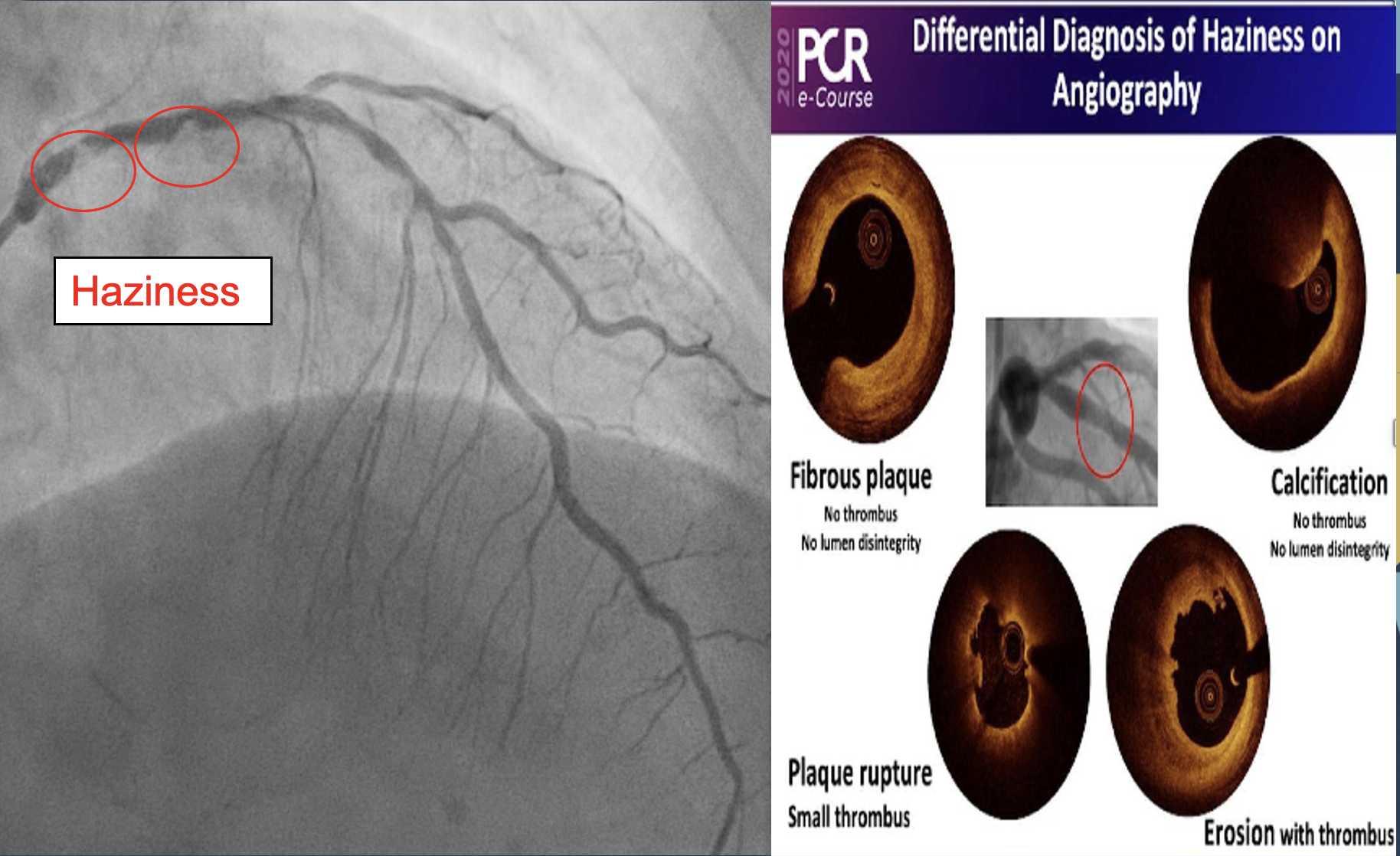
Very short left main. There were ambiguous lesion in proximal LAD which appeared as hazy severe eccentric stenosis. The LCx was normal. The RCA demonstrated severe calcification.
Interventional Management
Procedural Step
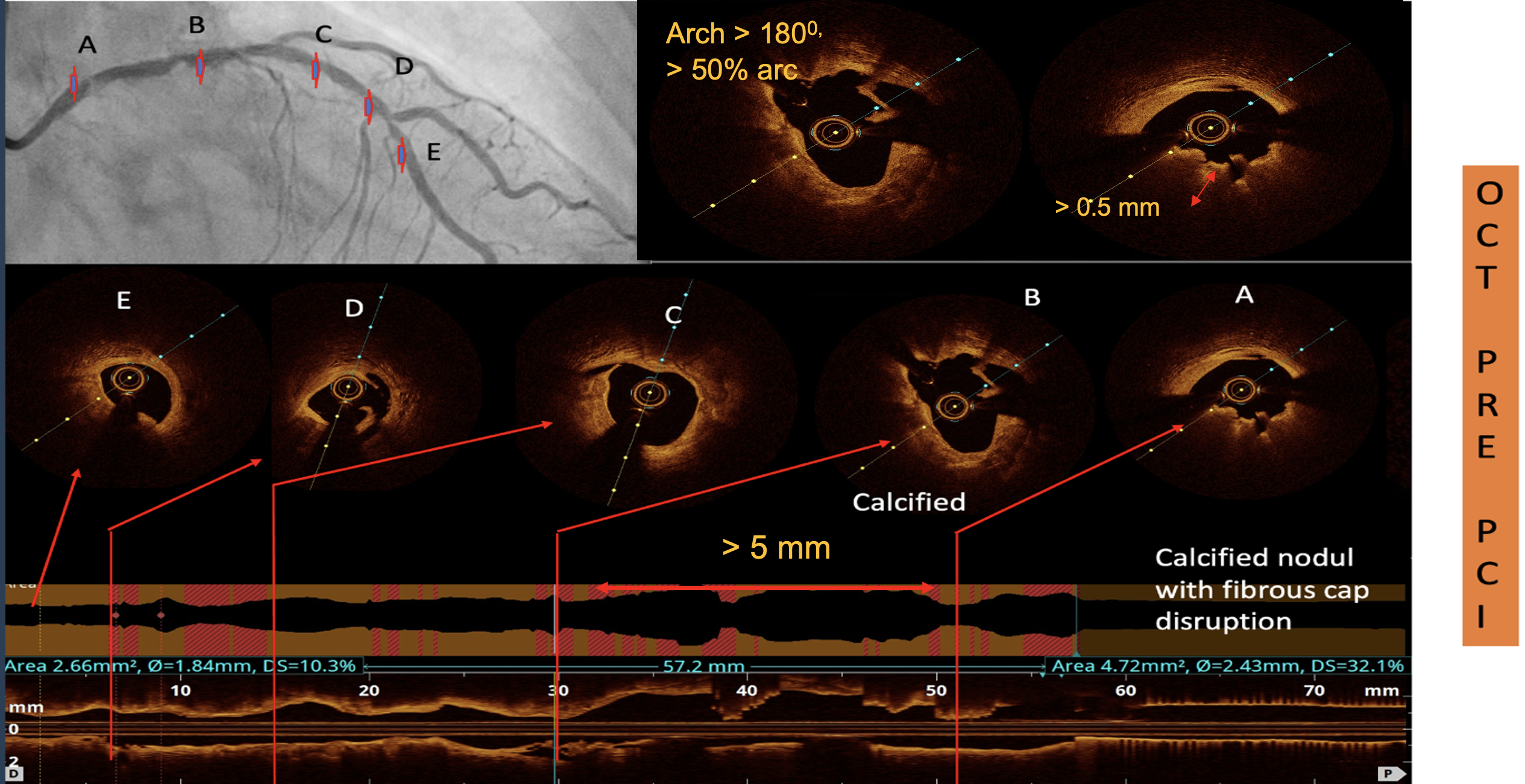
A 7Fr JL 3.5 guiding catheter was engaged into LCA ostium. Base on her ECG, we decided to do early invasive strategy to LAD which we considered as the culprit vessel. Following predilation using 2.0 x 15 mm semi compliance balloon,OCT was used to guide lesion preparation. OCT showed eruptive calcified nodule with fibrous cap disruption at haziness area, calcified lesion with arc > 270 0, Calcium Volume Index Score was 4.Based on OCT result we decided to do rotablation. Rotablation with 2.0 mm burr done with 180.000 rpm. Additional lesion preparation using 2.5 x 15 mm Scoring Balloon inflate up to 18 atm. GW Runthrough floppy was placed to D2 as jailed wire. Two overlapping 2.5 x 38 mm and 3.0 x 33 mm DES were implanted at mid-proximal LAD. OCT evaluation post stenting showed under expansion stent and there were malapposition and proximal LAD. We decided to optimize the implanted stent using 2.5 x 15 mm balloon at mid and 3.5 x 12 mm Non Compliance Balloon (NCB) at proximal. OCT evaluation showed there was good expansion (MSA 5.84 mm), but there was mal apposition at proximal part, then NCB 3.5 x 12 mm delivered and inflate high pressure. FinalAngiogram showed good result with TIMI 3 Flow.
Case Summary
Calcified nodule recognized as one of the underlying mechanisms of acute coronary syndrome (ACS). It could impact on stent deployment. Intracoronary imaging usage is very crucial to determine the ambiguous lesion in ACS and to strategize the planning and optimizing PCI. Rotational atherectomy should be considered as the treatment of calcified nodule in ACS.