
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-143
Mesenteric Venous Thrombosis With Abdominal Compartment Syndrome
By Chao Yun Cheng
Presenter
Chao-Yun Cheng
Authors
Chao Yun Cheng1
Affiliation
National Cheng Kung University Hospital, Taiwan1,
View Study Report
TCTAP C-143
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Mesenteric Venous Thrombosis With Abdominal Compartment Syndrome
Chao Yun Cheng1
National Cheng Kung University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Mr. Chen
Relevant Clinical History and Physical Exam
This a 63-year-old male was general well before until he had post-prandial lower abdominal pain for 5 days. Therefore, he presented himself to the emergency department of National Cheng Kung University Hospital. Remarkable physical examination revealed hypoactive bowel sound and lower abdominal tenderness without peritoneal sign.

Relevant Test Results Prior to Catheterization
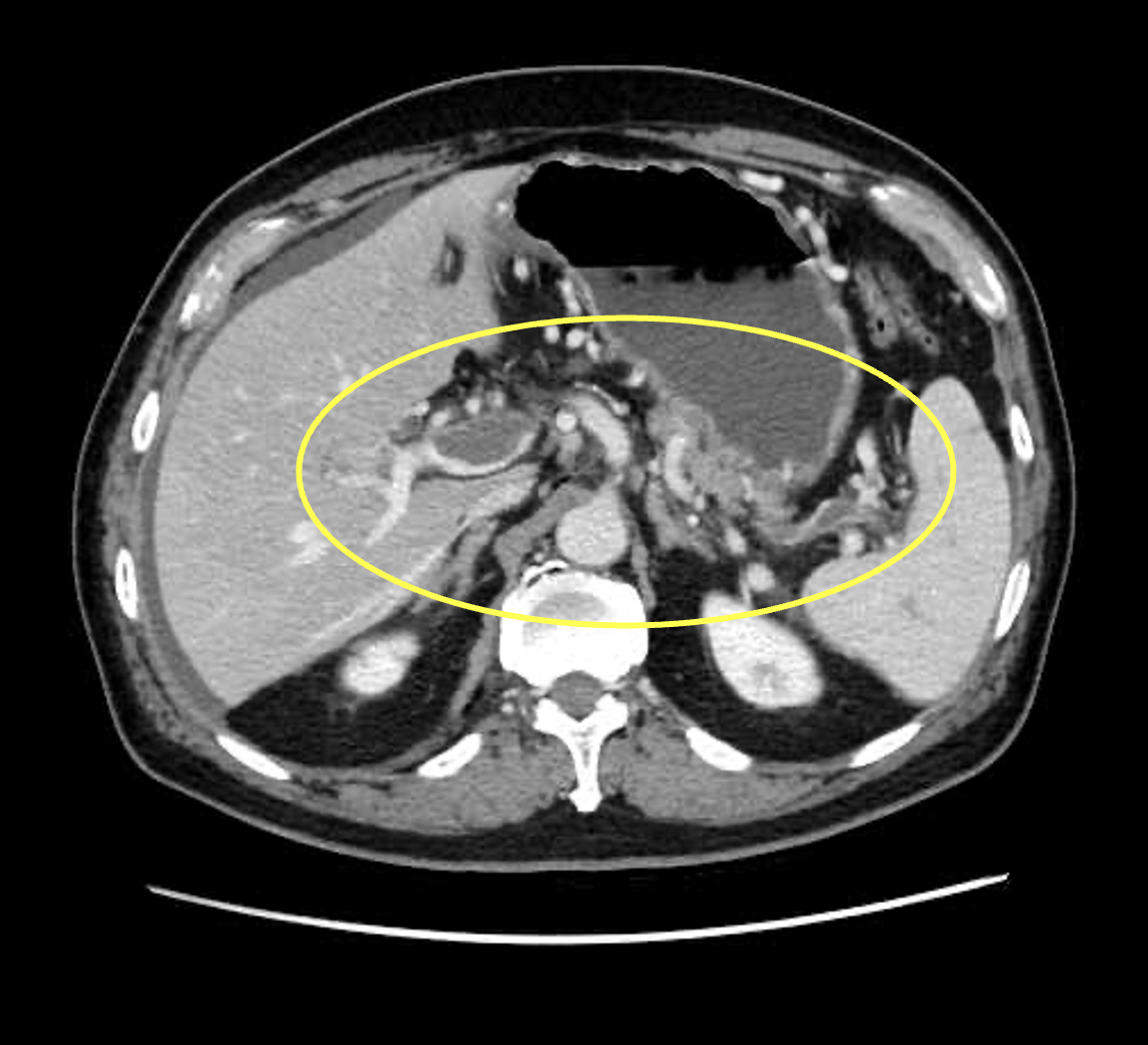
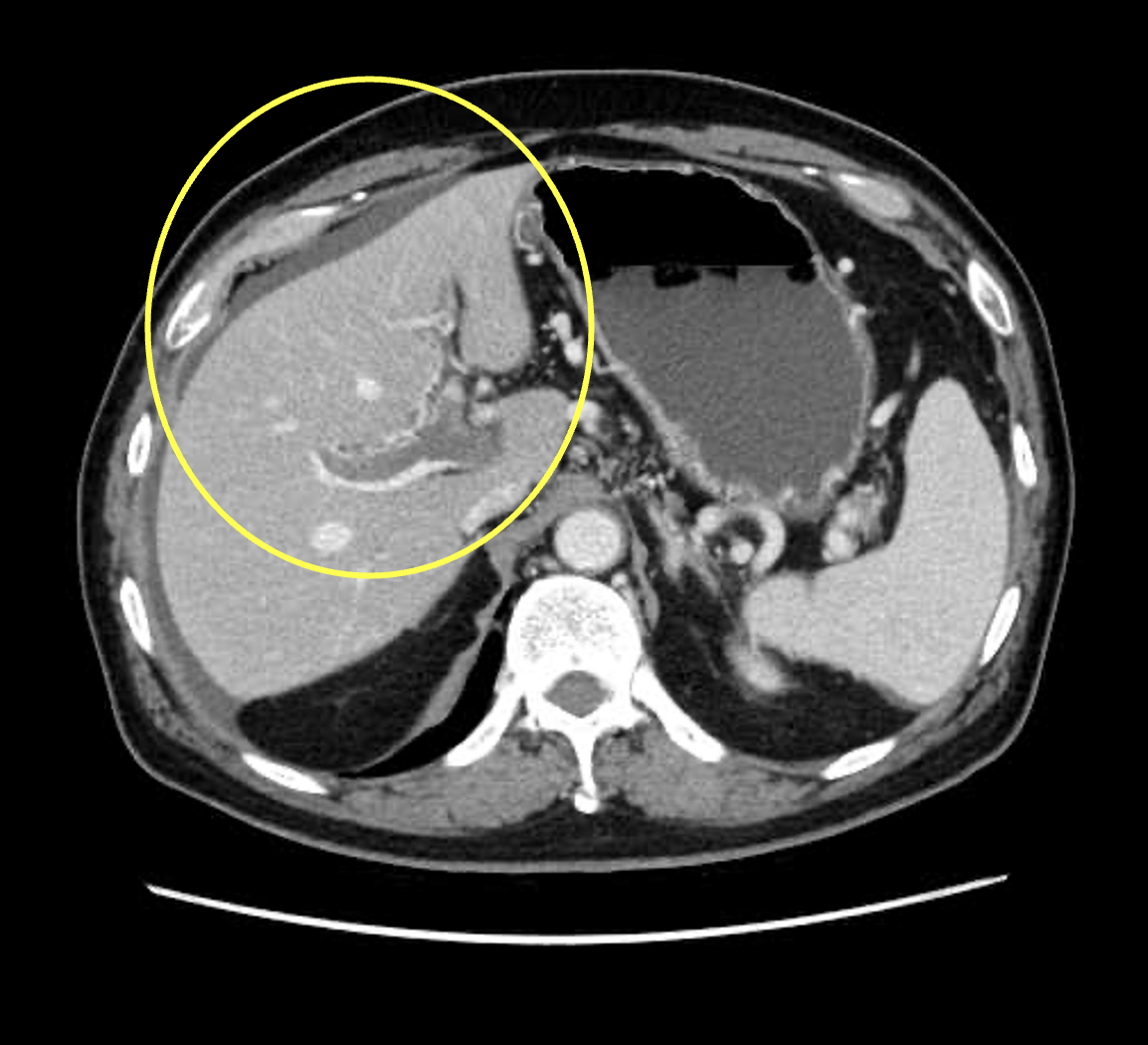
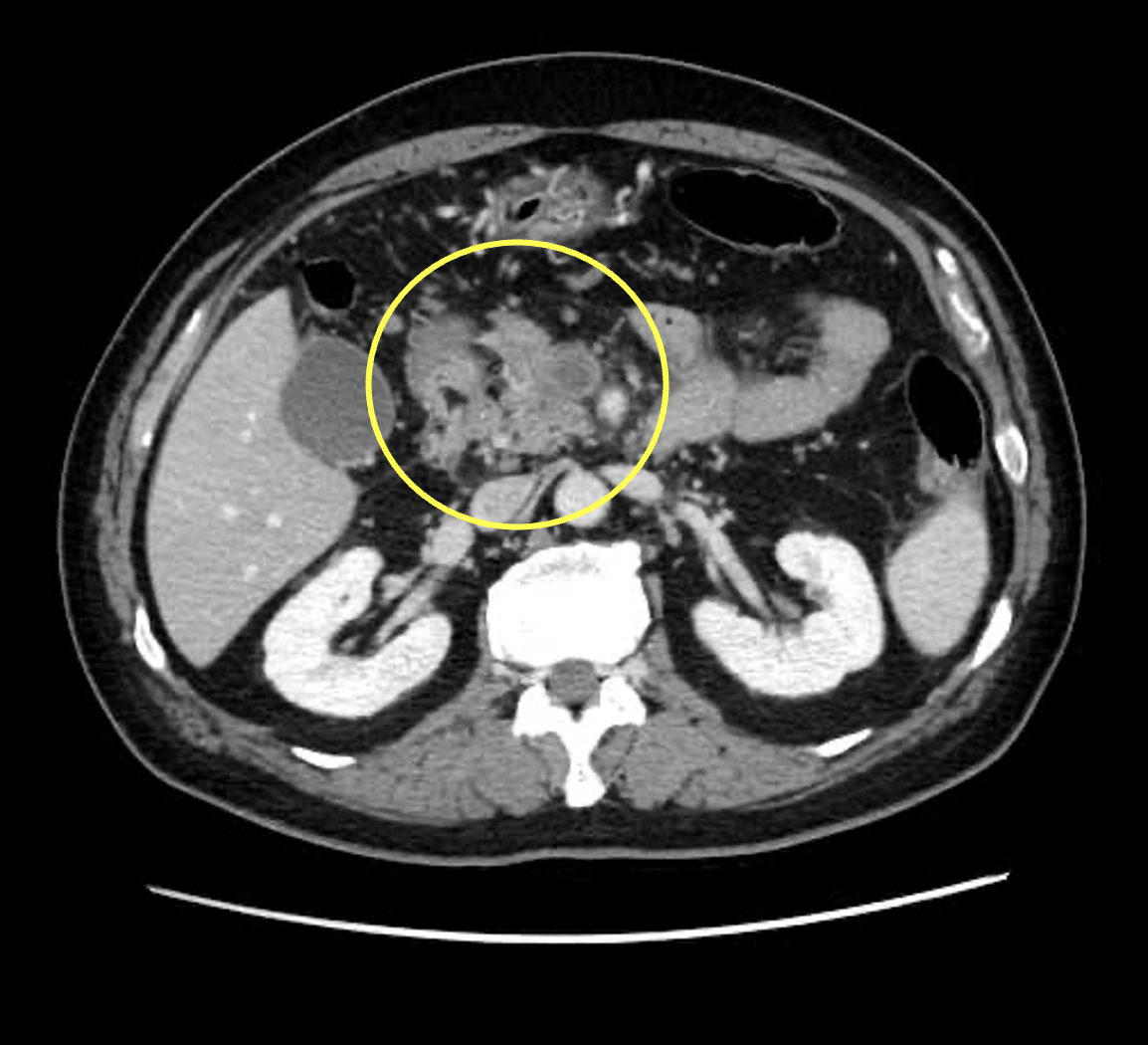
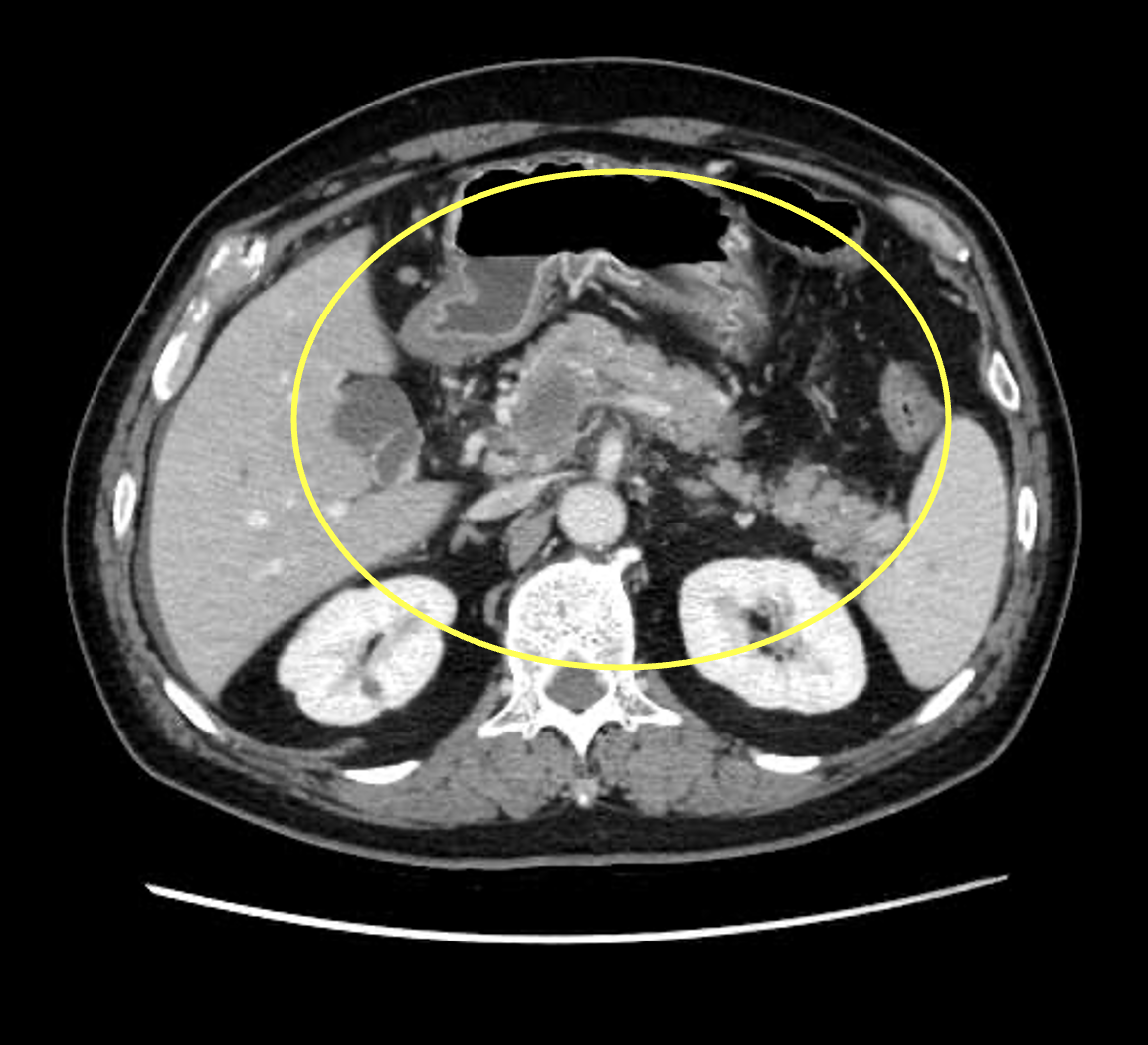
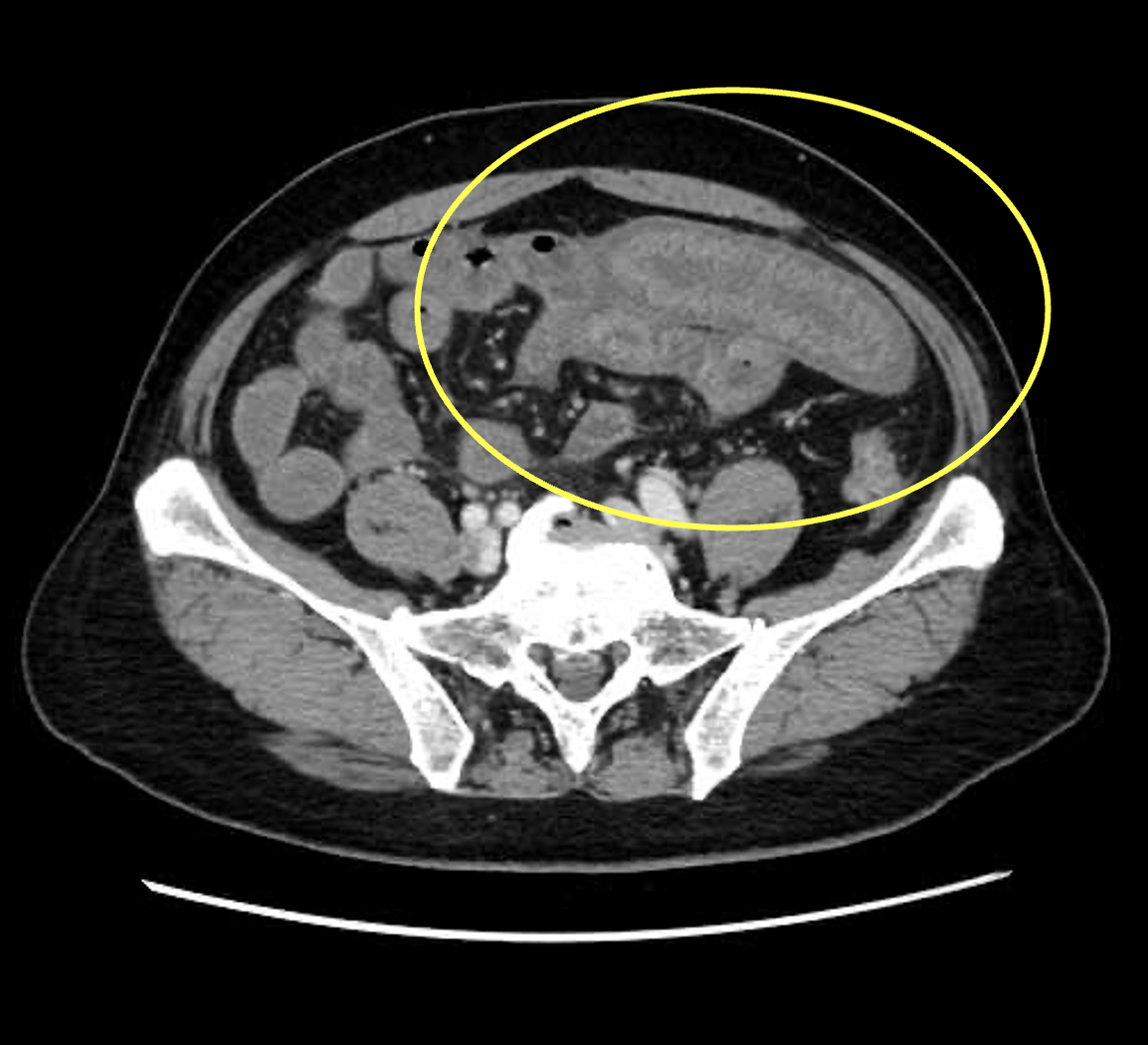
He had leukocytosis with elevating white blood cell count 18.8*103/μL, renal function impairment with increasing creatine level up to 2.77 mg/dL and lactate acidosis (increasing lactate acid 5.7mmol/L). Abdominal computed tomography scan with contrast showed diffuse portal and mesenteric system thrombosis with intestinal edematous change and small amount ascites formation. Under impression of diffuse portal and mesenteric system thrombosis, he was admitted to the intensive care unit.
Relevant Catheterization Findings
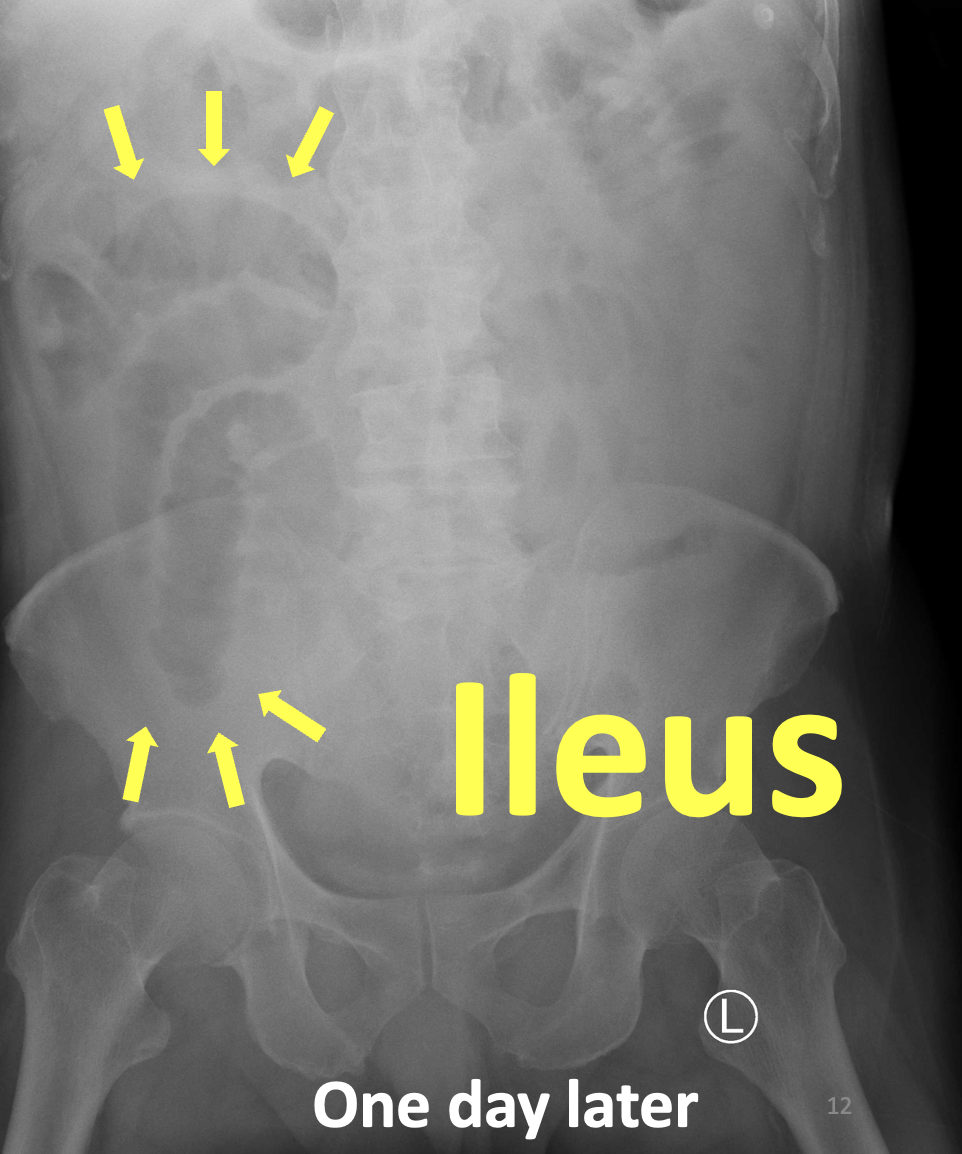
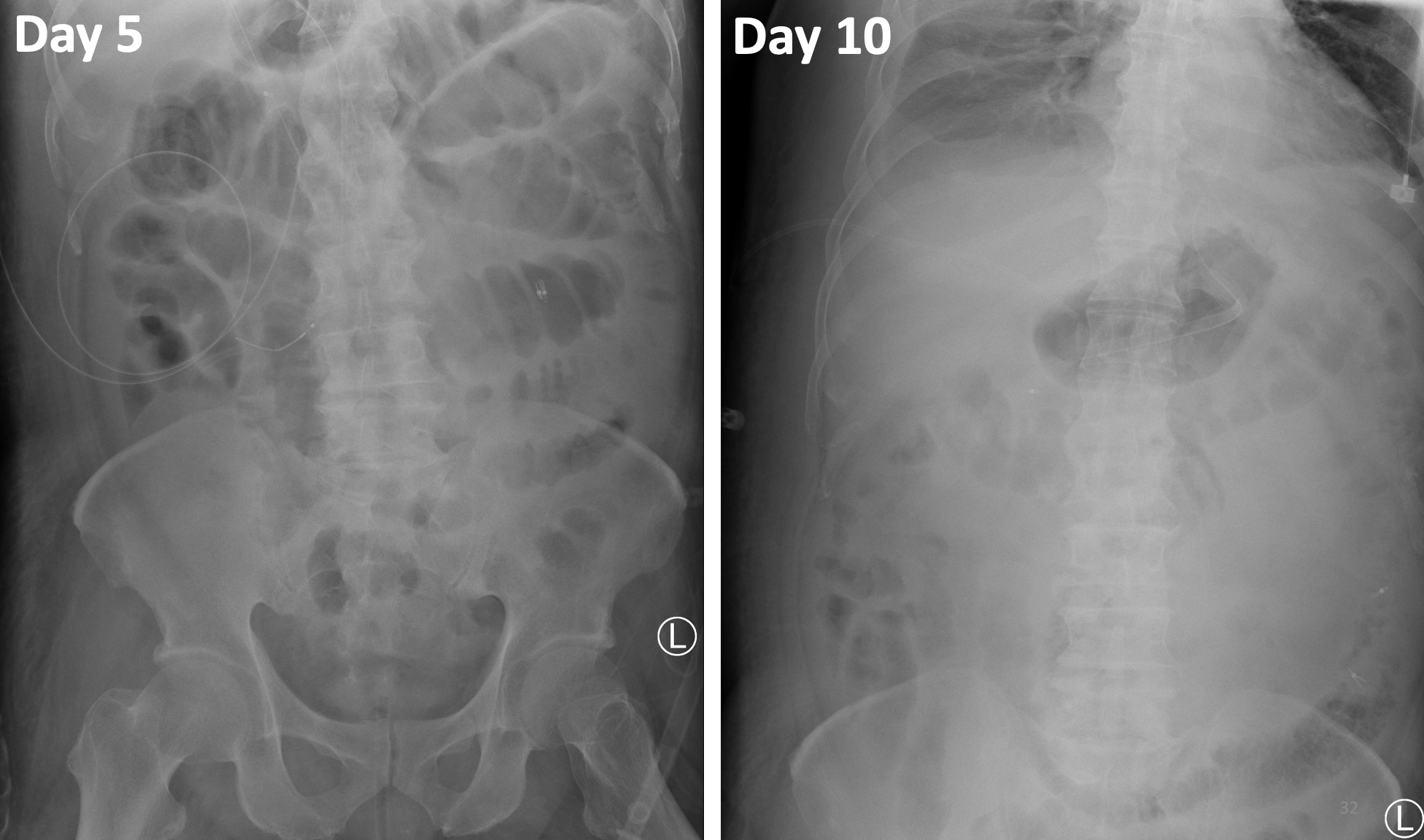
A general surgeon suggested conservative treatment with antibiotics and heparin use. In the next day, he had decreasing urine output with simultaneously increasing intraabdominal pressure up to 26mmHg. Portable abdominal x ray showed progressive ileus. For abdominal compartment syndrome, he underwent endovascular intervention. The 5 French sheath advanced to right main portal vein via ultrasound-guided percutaneous transhepatic access. The angiography showed massive thrombus in portal vein and SMV.

 day 1.wmv
day 1.wmv
Interventional Management
Procedural Step
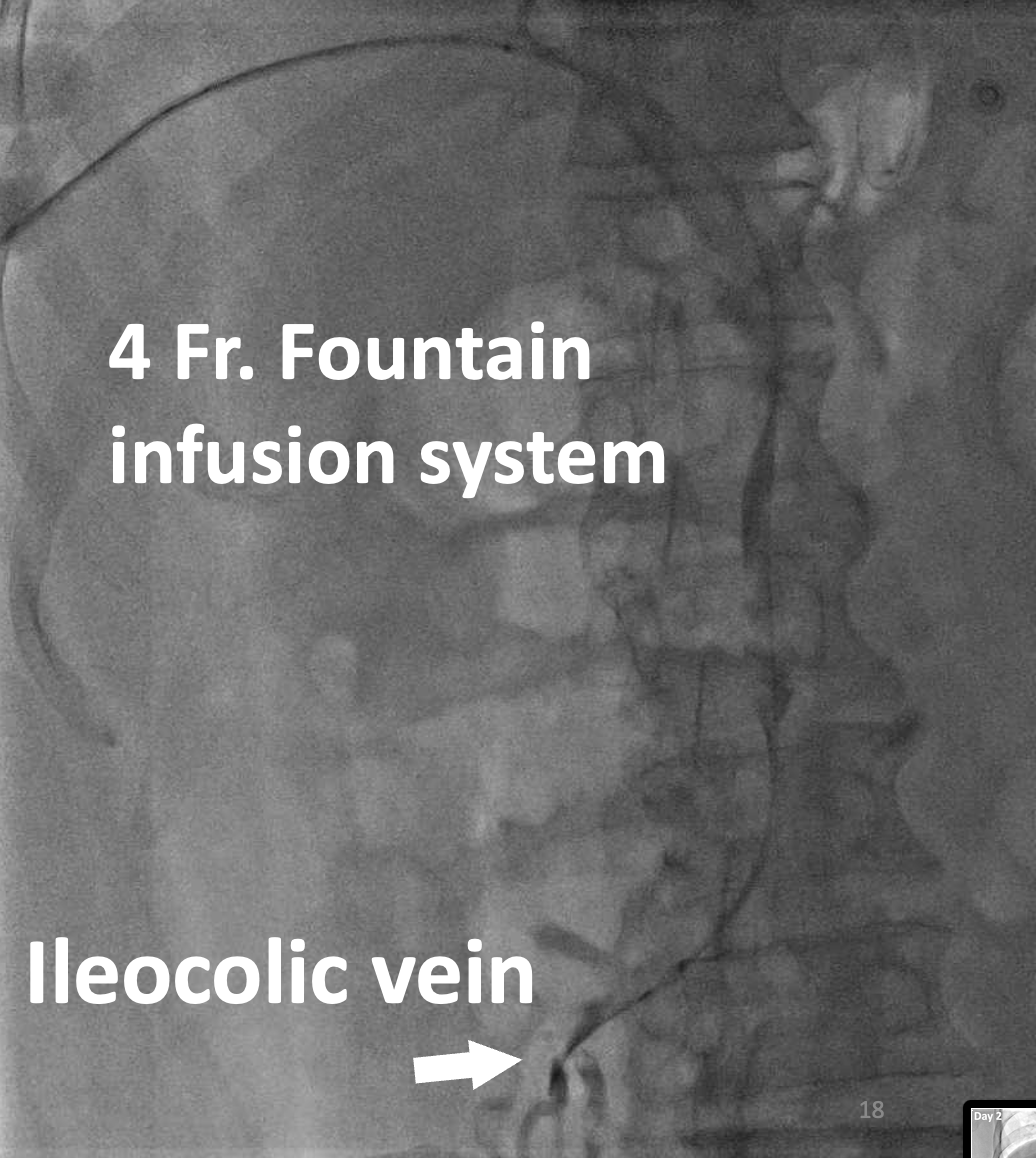
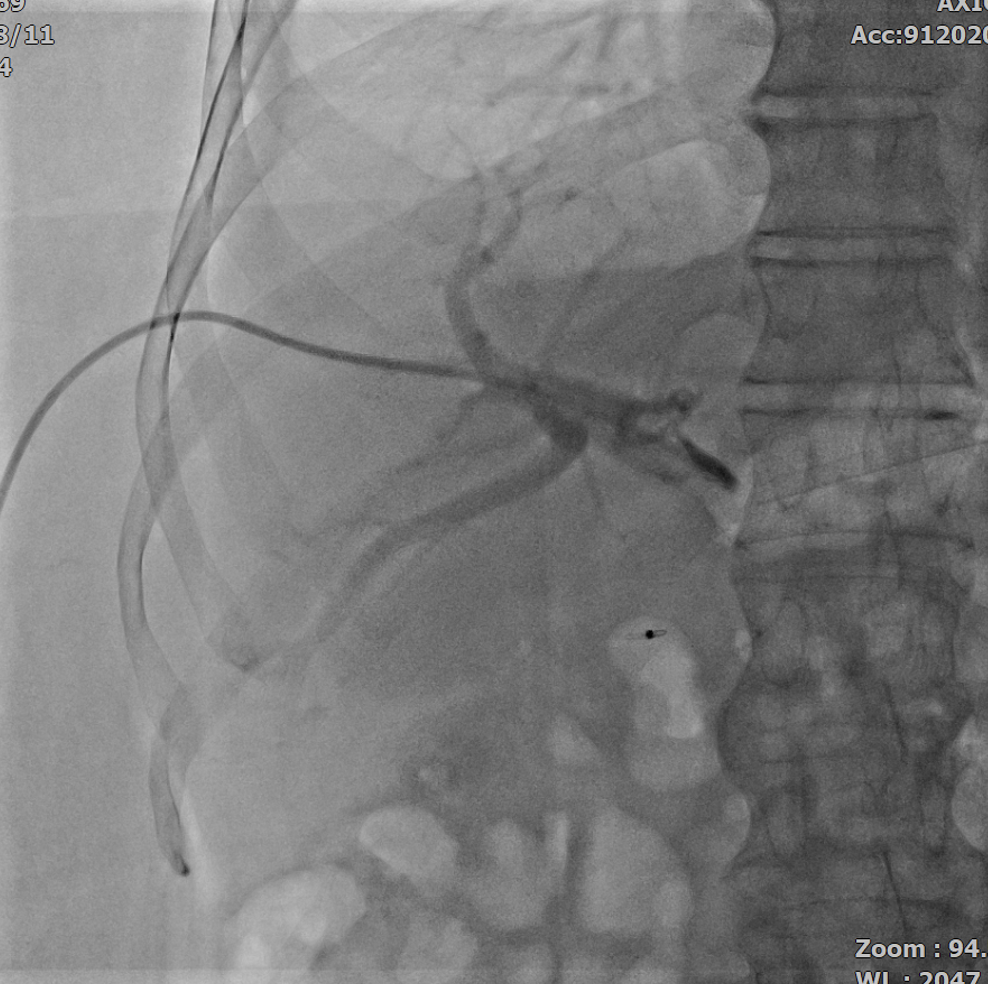
Terumo wire advanced to distal ileocolic vein. Percutaneous transhepatic portal and mesenteric thrombolysis with 4 French fountain catheter urokinase (60,000 unit per hour) infusion system was performed. However, active upper gastro-intestinal bleeding due to gastric ulcer developed and thus we hold urokinase infusion. Two days later, follow up angiography showed thrombus partial remission. We resumed urokinase infusion gradually since day four of admission. No more bleeding was noted in the following days. Percutaneous trans-hepatic thrombectomy with Angiojet and non-compliant balloon angioplasty were performed for still residual thrombus at portal and mesenteric system when follow up. Much residual thrombus was removed and urokinase thrombolysis was kept using. He regained his normal renal function and started to have oral intake on day seven of admission. Finally, angiography showed only some small residual thrombus and the venous return flow to central vein system was adequate. We performed right main portal vein tract coil embolization smoothly after infusion catheter removal. He was transferred from ICU to GI wards on day ten of admission.However, he had ischemia bowel due to recurrent portal and mesenteric system thrombosis suspect related to inadequate dose of anticoagulant. He refused surgical laparotomy and any other invasive intervention. Unfortunately, he expired from septic shock a couple of days later.
final 3.wmv
final 2.wmv
final1.wmv
day 6 angioplasty.wmv
day 4 follow up.wmv
day 7 angioplasty.wmv
day 7 result.wmv
day 6 follow up.wmv
day 6 result2.wmv
day 6 result1.wmv
day 6 angiojet.wmv

Case Summary
Lactate acidosis and intra-abdominal pressure are clinical important guidance of portal and mesenteric vein thrombosis progression.