
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-007
Extracorporeal Membrane Oxygenation Supported Intravascular Ultrasound Guided Multi Vessel Angioplasty Involving Left Main and Left Anterior Descending Artery
By Arindam Pande
Presenter
Arindam Pande
Authors
Arindam Pande1
Affiliation
Apollo Gleneagles Hospital Ltd., India1,
View Study Report
TCTAP C-007
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Extracorporeal Membrane Oxygenation Supported Intravascular Ultrasound Guided Multi Vessel Angioplasty Involving Left Main and Left Anterior Descending Artery
Arindam Pande1
Apollo Gleneagles Hospital Ltd., India1,
Clinical Information
Patient initials or Identifier Number
SKD
Relevant Clinical History and Physical Exam
73-year-old male with known case of interstitial lung disease (ILD) admitted with complaint of comprehensive central chest pain for 3-4 days. Patient was hypertensive and suffering from diabetes mellitus. His BP was 160/100. HR 80 beats/min.
Relevant Test Results Prior to Catheterization
ECG : NSTEMI
ECHO : No RWMA, LVEF : 60%
Trop T - Positive
ECHO : No RWMA, LVEF : 60%
Trop T - Positive
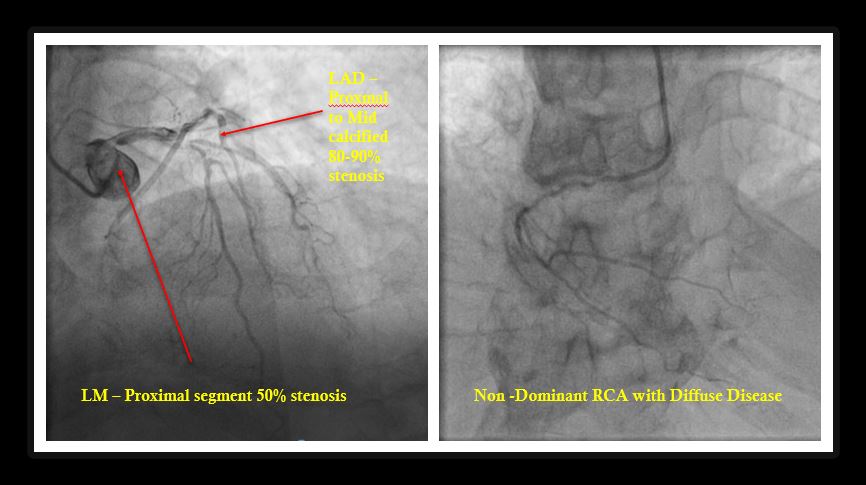
Relevant Catheterization Findings
Left Main : Proximal Segment has 50% stenosis
LAD / Diagonal : Proximal to mid calcified 80-90% stenosis
RAMUS INTERMEDIUS : NA
LCX/OM : Co-dominant. Proximal calcified 40-50% stenosis, OM1 - 50-60% stenosis
RCA : Co-dominant, Diffuse Critical Stenosis
Final Diagnosis : Triple Vessel Coronary Artery Disease with LMCA stenosis.
LAD / Diagonal : Proximal to mid calcified 80-90% stenosis
RAMUS INTERMEDIUS : NA
LCX/OM : Co-dominant. Proximal calcified 40-50% stenosis, OM1 - 50-60% stenosis
RCA : Co-dominant, Diffuse Critical Stenosis
Final Diagnosis : Triple Vessel Coronary Artery Disease with LMCA stenosis.
Interventional Management
Procedural Step
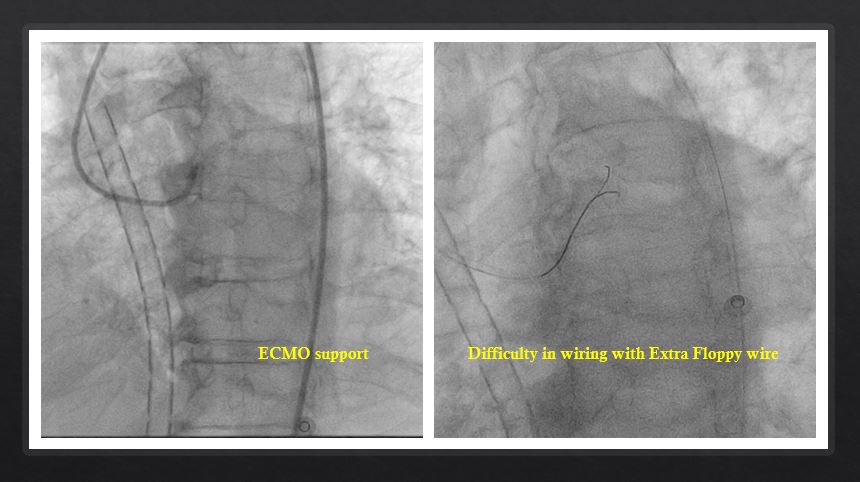
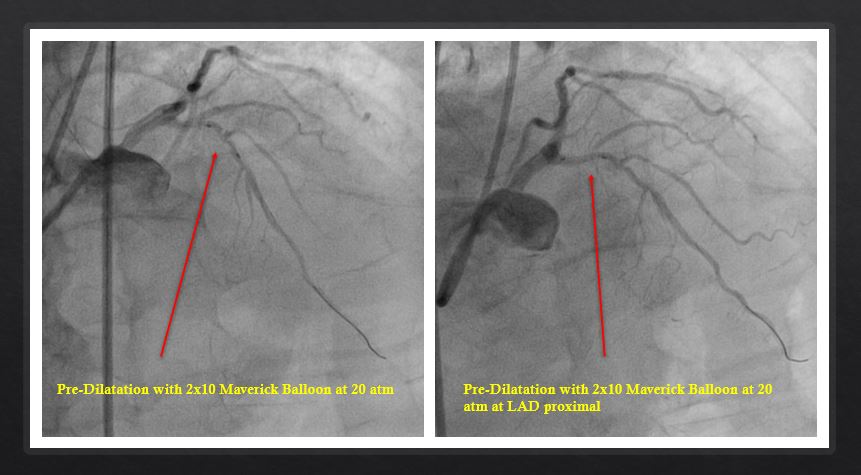
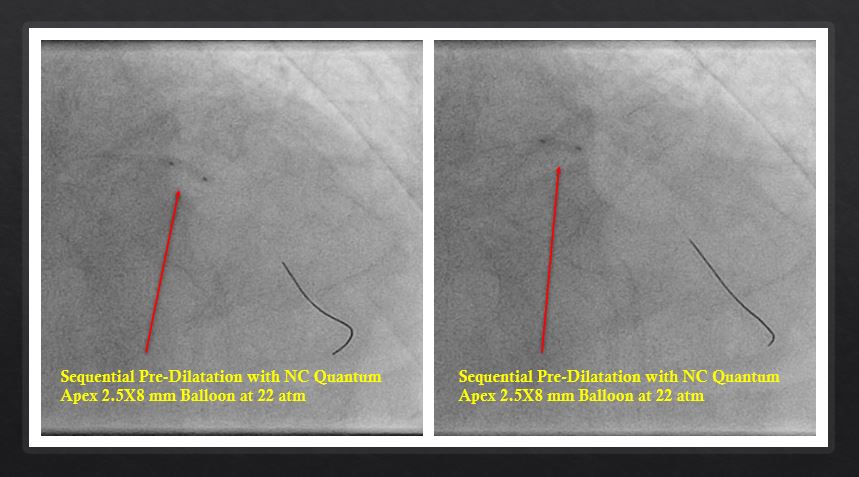
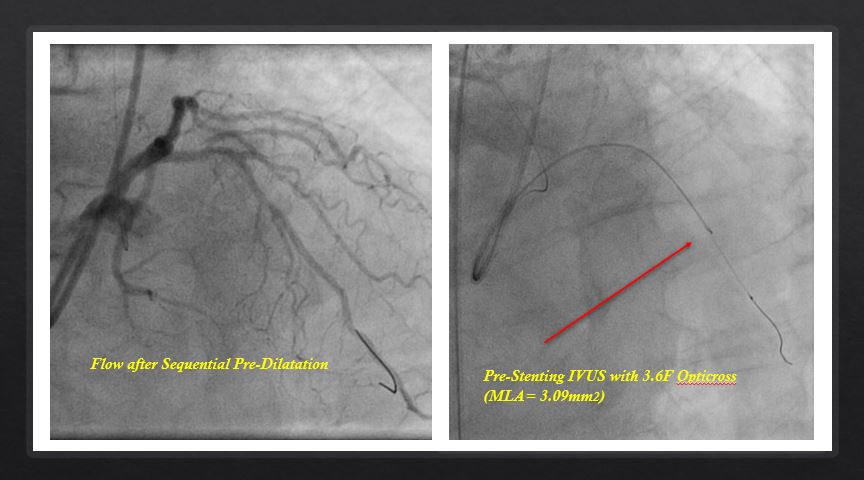
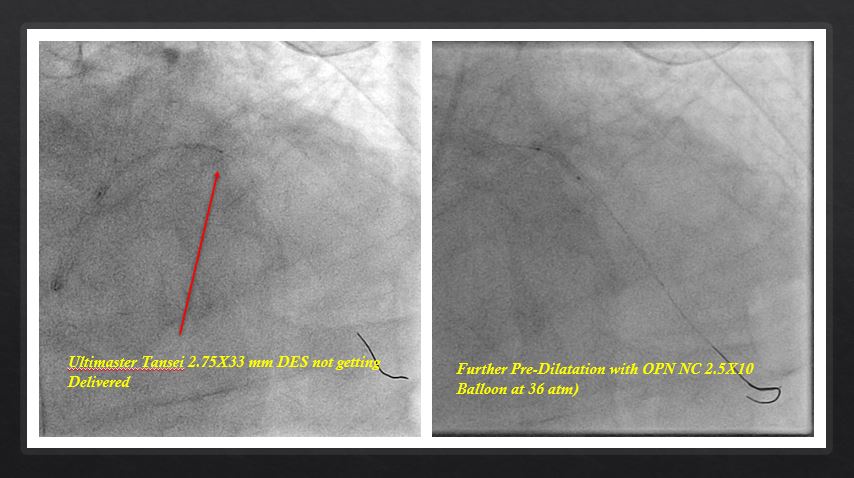
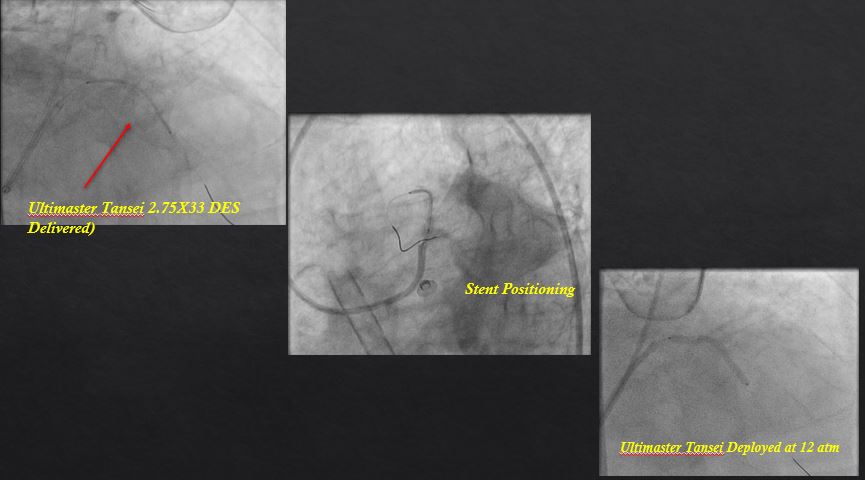
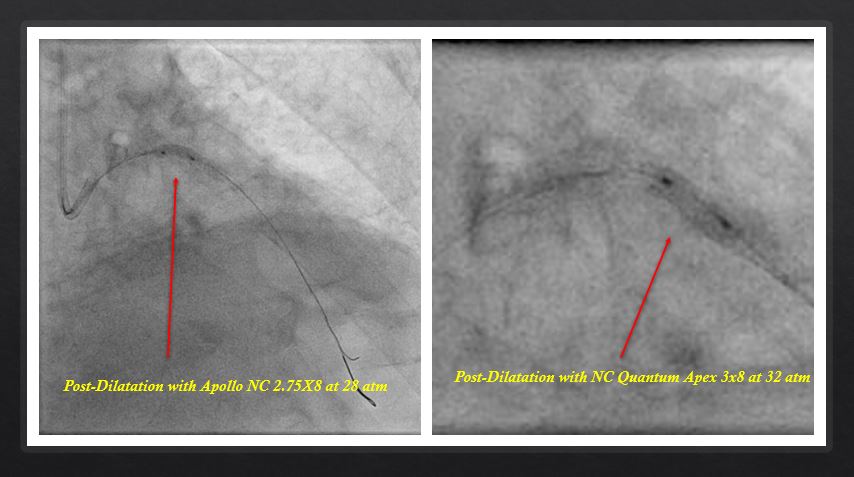
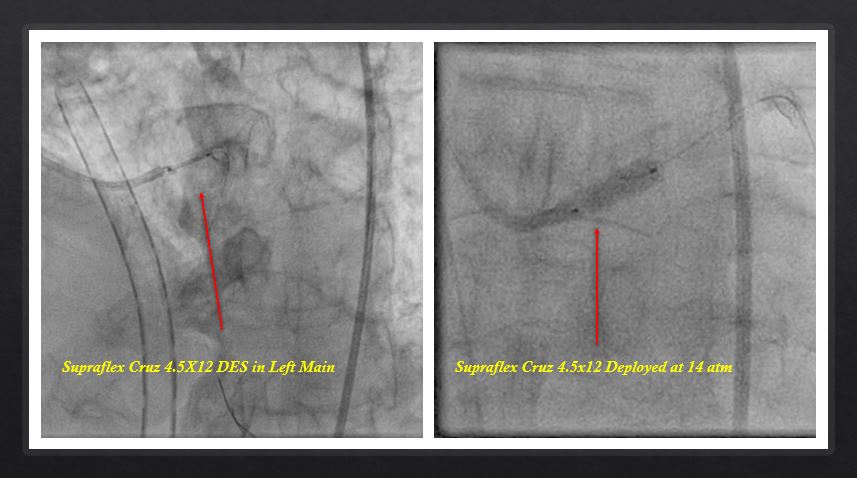
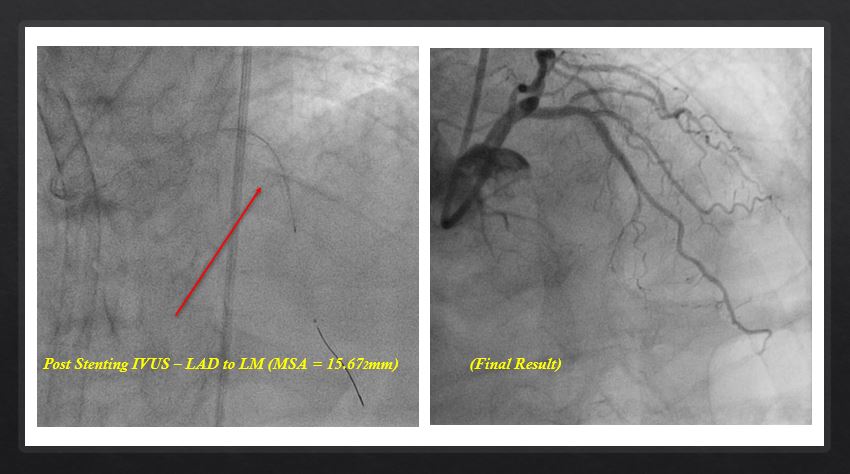
PTCA was done through right femoral approach. 7FJL3.5 guide catheter was used to engage the left coronary artery. Extrafloppyguide wire was taken to cross the lesion. Sequential pre-dilatation was donewith Maverick 2x12 SC balloon at 20 atm and followed by NC Quantum Apex 2.5X8mm balloon at 22 atm. We tried to deliver Ultimaster Tansei 2.75X33 mm DES andfailed to deliver. Further pre-dilatation was done with OPN NC 2.5X10 balloonat 36 atm. Pre-stenting IVUS run performed with 3.6F Opticross and MLA derived3.09mm2. Ultimaster Tansei 2.75X 33 mm DES deployed at LAD at 12 atm.Sequential boost guided post-dilatation done with Apollo NC 2.75X8 mm at 28 atmand followed by NC Quantum Apex 3x8 mm at 32 atm. Direct stenting to LMCAostium was done with Supraflex Cruz DES 4.5X12 at 14atm. Flaring done by samestent balloon at 16 atm. Final IVUS done to LMCA with 3.6F Opticross (MSA =15.67mm2). Post Procedure TIMI III flow was achieved.
 Final Result RUN.avi
Final Result RUN.avi
Case Summary
ECMO supported angioplasty as patient had a history of interstitial lung disease in ACS condition is high risk procedure as LMCA and LAD was involved. Proper planning and proper hardwire selection are extremely important for an uneventful procedure.