
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-102
Management and Retrieval of Undeflatable Non-compliant Coronary Balloon During Percutaneous Coronary Intervention
By Arvin Romero Yumul, Shaiful Azmi Yahaya, Kumara Gurupparan Ganesan, Jayakhanthan Kolanthaivelu, Faten Aqilah Aris, Mohamed Nazrul Mohamed Nazeeb, Khin Maung Zan Mohd Saad Jalaluddin, Chee Sin Khaw
Presenter
Arvin Romero Yumul
Authors
Arvin Romero Yumul1, Shaiful Azmi Yahaya2, Kumara Gurupparan Ganesan2, Jayakhanthan Kolanthaivelu3, Faten Aqilah Aris2, Mohamed Nazrul Mohamed Nazeeb2, Khin Maung Zan Mohd Saad Jalaluddin4, Chee Sin Khaw5
Affiliation
Medical Center Manila, Philippines1, National Heart Institute, Malaysia2, Cardiovascular Sentral Kuala Lumpur, Malaysia3, Hospital Pusrawi, Malaysia4, Sunway Medical Centre Penang, Malaysia5,
View Study Report
TCTAP C-102
CORONARY - Complications
Management and Retrieval of Undeflatable Non-compliant Coronary Balloon During Percutaneous Coronary Intervention
Arvin Romero Yumul1, Shaiful Azmi Yahaya2, Kumara Gurupparan Ganesan2, Jayakhanthan Kolanthaivelu3, Faten Aqilah Aris2, Mohamed Nazrul Mohamed Nazeeb2, Khin Maung Zan Mohd Saad Jalaluddin4, Chee Sin Khaw5
Medical Center Manila, Philippines1, National Heart Institute, Malaysia2, Cardiovascular Sentral Kuala Lumpur, Malaysia3, Hospital Pusrawi, Malaysia4, Sunway Medical Centre Penang, Malaysia5,
Clinical Information
Patient initials or Identifier Number
Z.M.A.
Relevant Clinical History and Physical Exam
We present a 56-year-old woman, a known case of hypertensive cardiovascular disease, type 2 diabetes mellitus and dyslipidemia. She was having intermittent episodes of angina on exertion and diagnosed with chronic coronary syndrome. She was started on anti-anginal regimen and advised to undergo additional tests.
Relevant Test Results Prior to Catheterization
On further work-up, 12-lead electrocardiogram showed non-specific ST-T wave changes and 2D echocardiogram showed a preserved left ventricular systolic function but with note of segmental wall motion abnormality suggestive of multi-vessel coronary artery disease. There was persistence of anginal symptoms despite optimal medical therapy hence she was advised to undergo coronary angiography.
Relevant Catheterization Findings
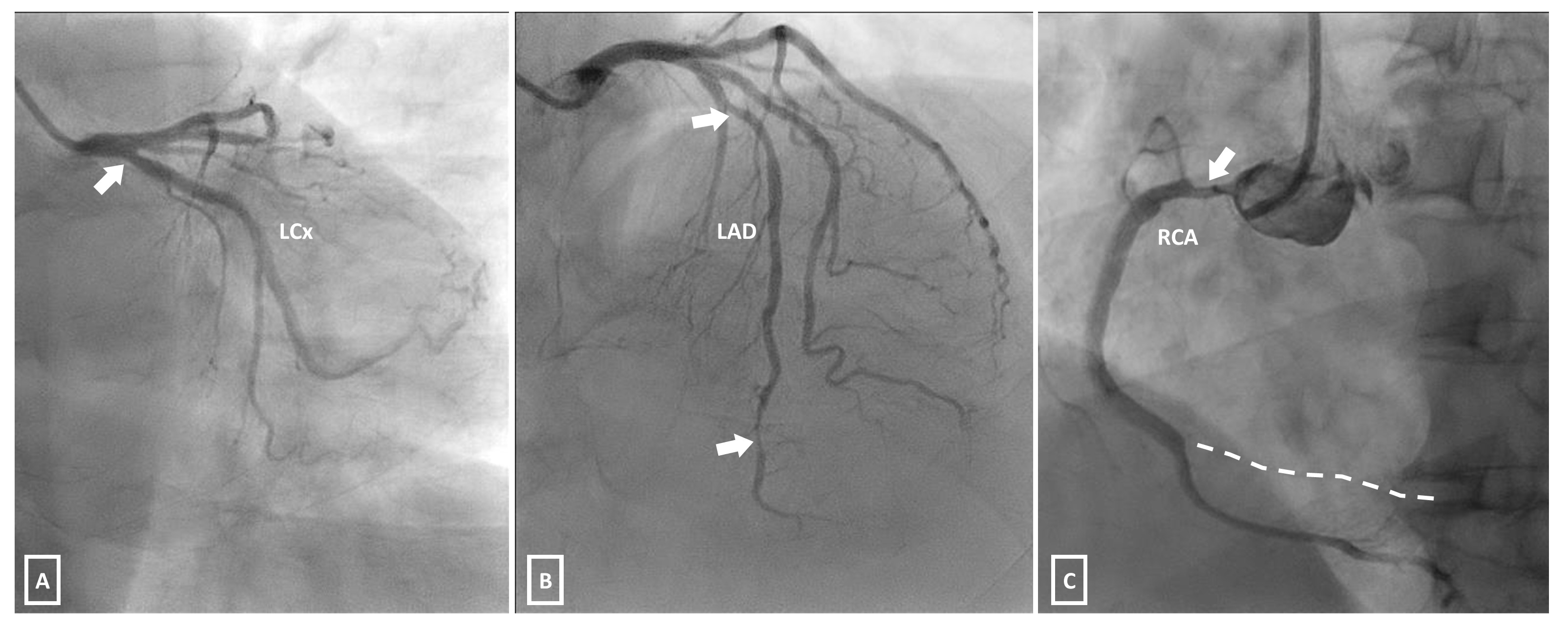
Diagnostic coronary angiogram showed moderate stenosis of the ostial left circumflex artery (image 1A), severe stenosis of the mid and distal left anterior descending artery (image 1B), and severe stenosis of the ostioproximal right coronary artery (RCA) and total occlusion of the posterior left ventricular artery (image 1C). Plan was to do a staged percutaneous coronary intervention (PCI) starting with the right coronary artery.
Interventional Management
Procedural Step
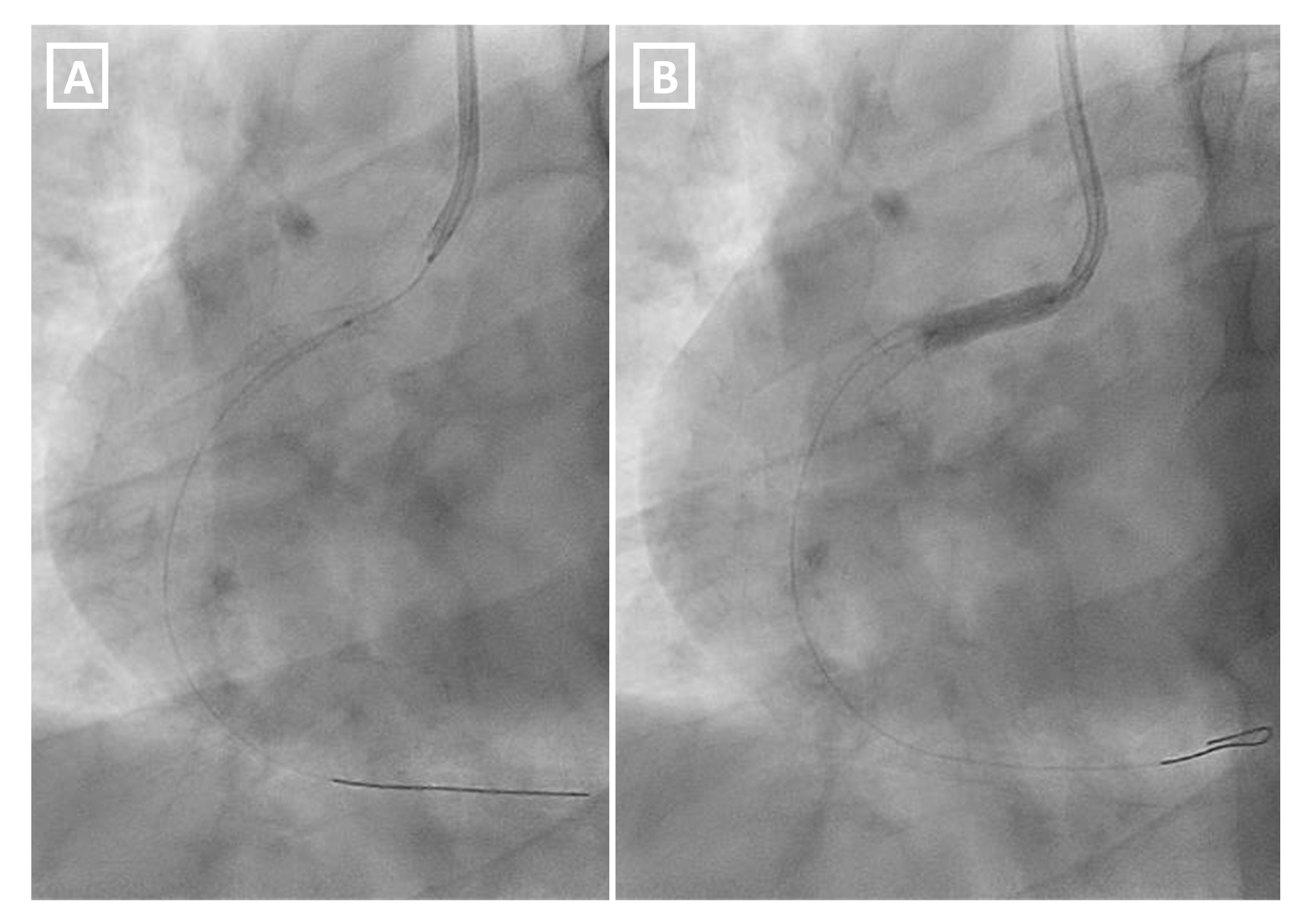
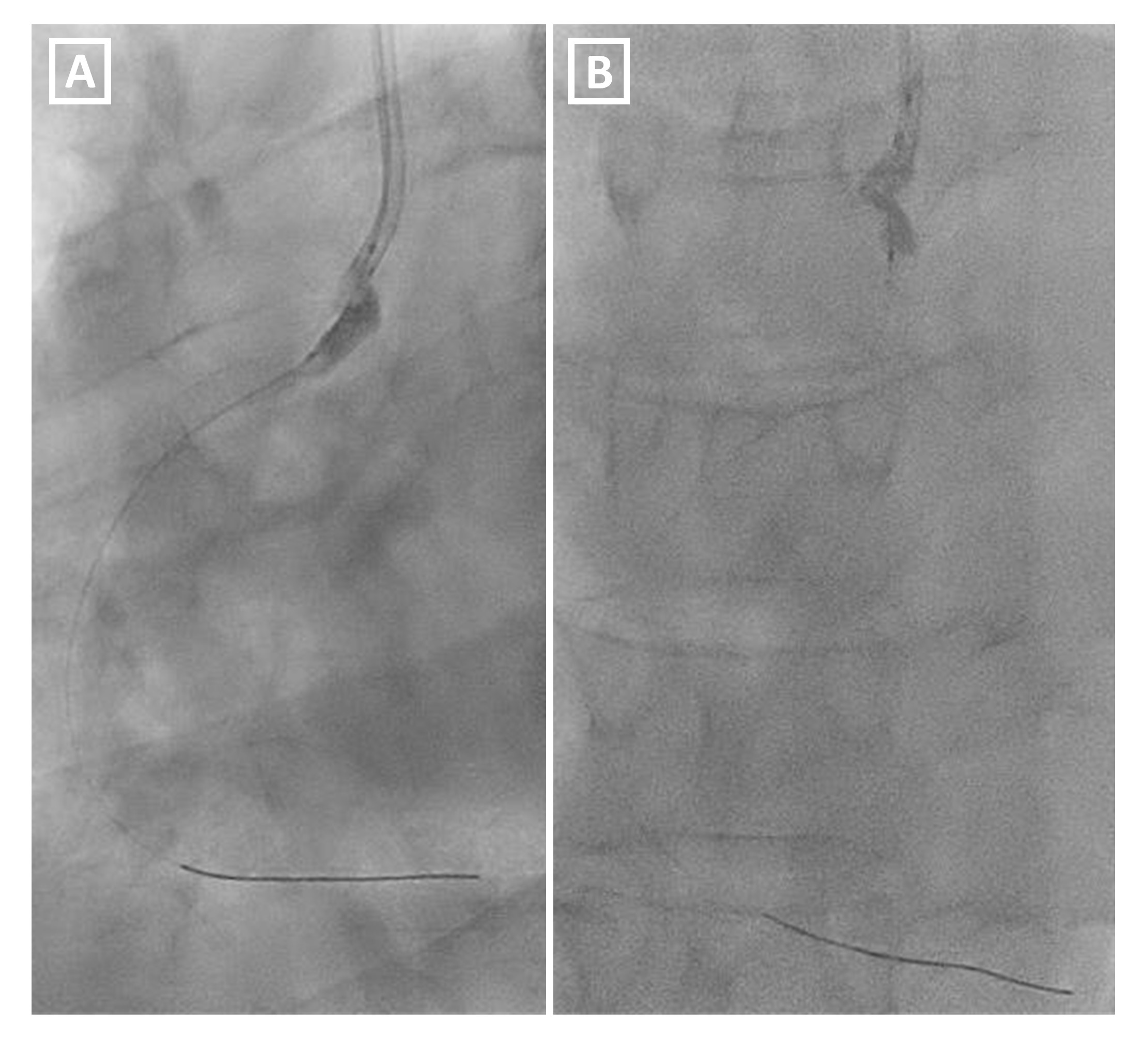
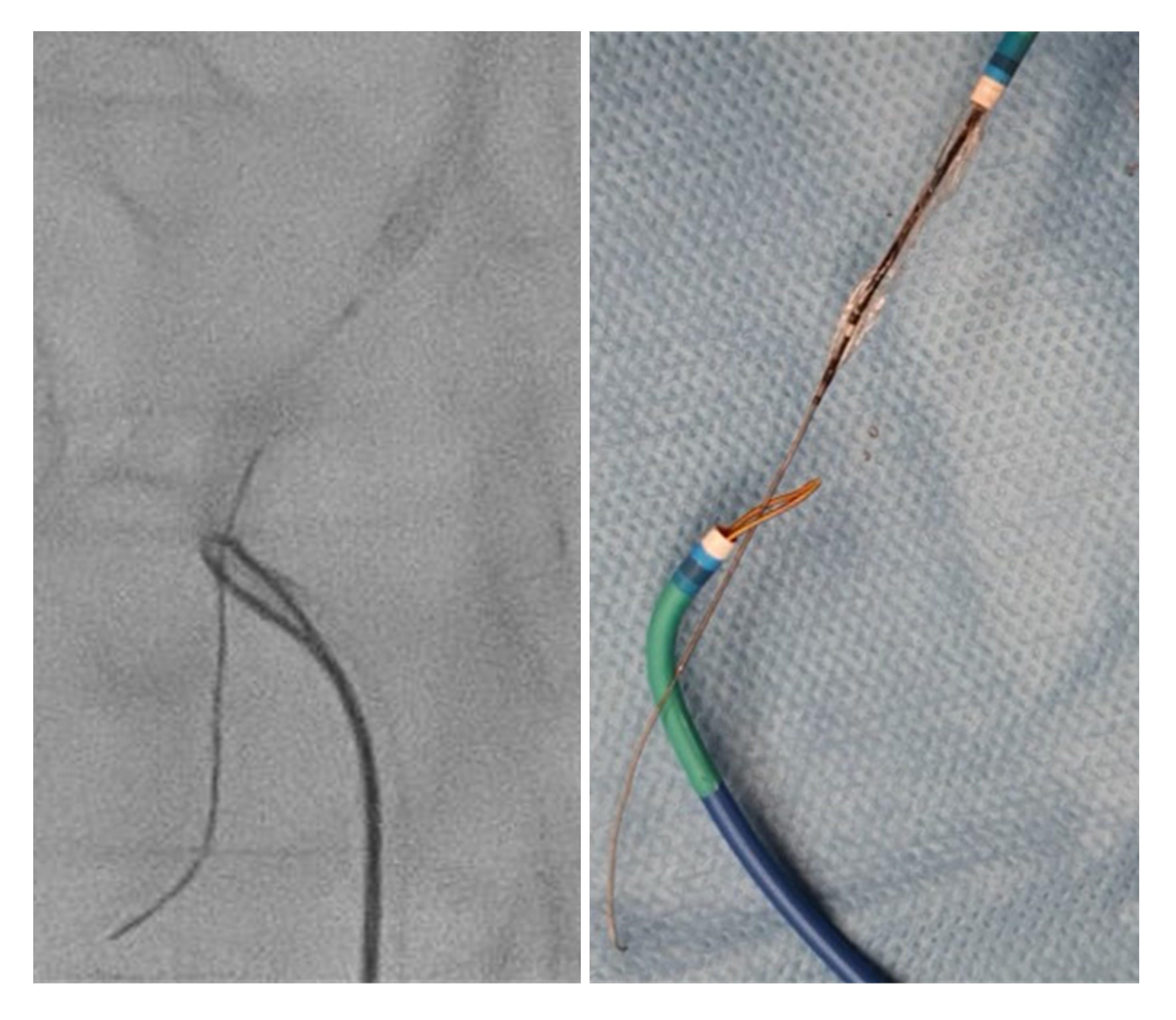
PCI of the RCA was done via right radial approach. Pre-dilatation of the ostioproximal RCA was done using a 4.0 x 15 mm scoring balloon at maximum of 16 atm. A 4.0 x 18 mm Zotarolimus-eluting stent was positioned at the aorto-ostial to proximal RCA and deployed at 20 atm. Post-dilatation was done using a 4.5 x 15 mm non-compliant (NC) balloon at maximum of 18 atm. There was difficulty in removing the fully-deflated NC balloon with resistance encountered at the proximal stent edge (image 2A), hence another inflation at 18 atm was done (image 2B). However, the balloon failed to deflate totally occluding flow. Despite replacing the indeflator and using pure saline, the balloon remained undeflatable. The patient started having chest pains with new onset ST-segment elevation. Multiple attempts to puncture the balloon using the stiff-end of the guidewire were unsuccessful. The balloon was then successfully deflated without causing any form of damage after intentionally bursting it by inflating to ultra-high pressure (image 3A). The balloon was deformed hence there was difficulty pulling it back inside the catheter (image 3B). The whole system was redirected and advanced into the abdominal aorta. A 6F One Snare system (Merit Medical Systems, Inc., Utah, USA) inserted via femoral approach was used to secure the distal edge of the balloon in order to straighten it by providing counter traction (image 4). The whole system was then safely removed via the radial sheath.
Case Summary
Undeflatable balloon is a rare and unpredictable complication during PCI which may lead to serious consequences. In our case, excessive stretching during pullback might have damaged the balloon and altered its mechanism. Fortunately, the inflation function remained intact and we were able to intentionally burst the balloon. Otherwise it would have been very difficult to deflate it using other proposed techniques since it involves the aorto-ostial segment of the RCA and there was ongoing chest pain with hemodynamic comprise. Deflating the balloon is one thing but retrieving it is another. The use of snare in this case was invaluable which prevented other possible complications.