
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-131
Fever and Hemoptysis as Rare Presenting Symptoms of Acute Aortic Dissection
By Tanveer Iqbal Penwala, Shaiful Azmi Yahaya, Mohd Nasir Muda
Presenter
Tanveer Iqbal Penwala
Authors
Tanveer Iqbal Penwala1, Shaiful Azmi Yahaya1, Mohd Nasir Muda1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-131
ENDOVASCULAR - Aorta Disease and Intervention
Fever and Hemoptysis as Rare Presenting Symptoms of Acute Aortic Dissection
Tanveer Iqbal Penwala1, Shaiful Azmi Yahaya1, Mohd Nasir Muda1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
Mr. RA
Relevant Clinical History and Physical Exam
55 year old gentleman with underlying diabetes, hypertension, dyslipidemia, coronary artery disease -post CABG 2016 and renal calculi presented with intermittent chest pain for one month. On admission , patient had persistent fever and recurrent hemoptysis in ward. He was admitted in another hospital 10 day before admission to our centre with similar complaint. He was given a course of IV antibiotic and had TB workup which was negative. Examination of lung and heart was unremarkable.
Relevant Test Results Prior to Catheterization
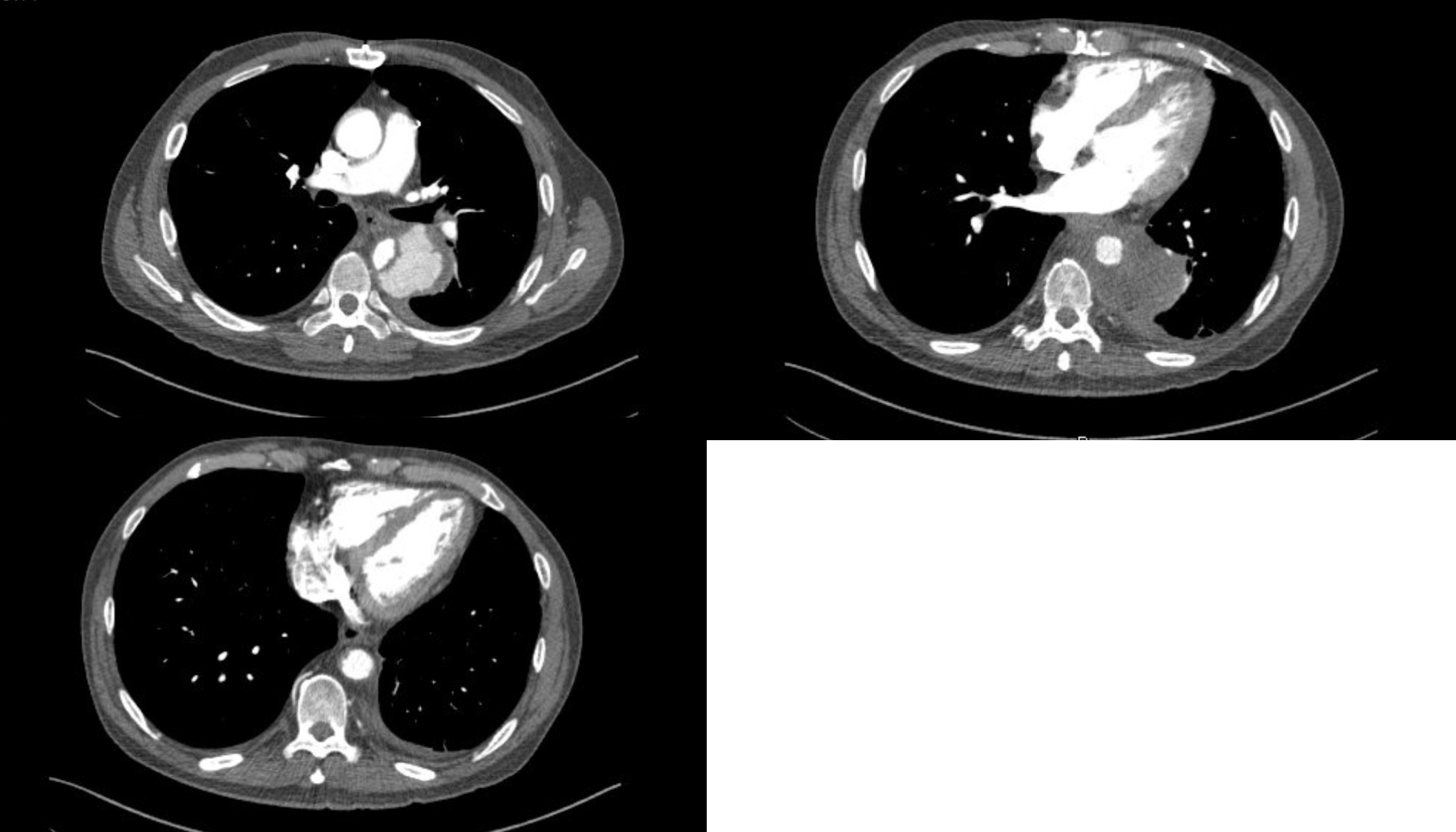
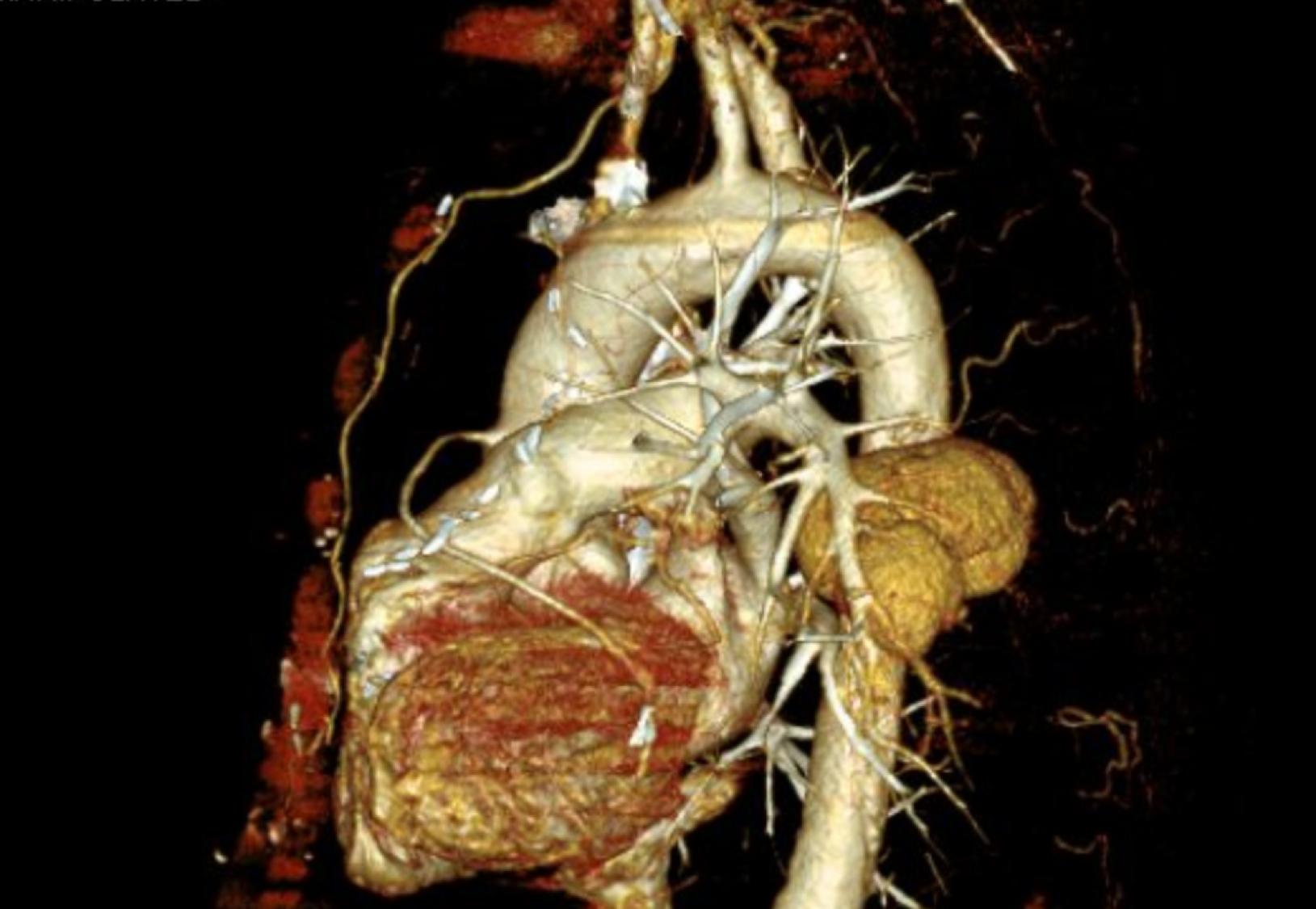
Cardiac enzymes were normal. ECG had T inversion V2-V5. MSCT graft study showed patent graft. Incidentally, a type B descending thoracic aortic aneurysm or dissection with hematoma was seen. CT angiogram showed concealed active leak of a focal aortic dissection in the descending thoracic aorta from just beneath carina until where the coronary sinus enters the right atrium. The leak was surrounded by thrombosed hematoma overall diameter 7.2x 8.0 x 7.2cm.There was aberrant right subclavian artery.
Relevant Catheterization Findings
Interventional Management
Procedural Step
Patient suddenly had massive hemoptysis the next day after CT angiogram was done. Due to the persistent fever, an impending mycotic aneurysm rupture was suspected. Patient was stabilized and brought to invasive cardiovascular lab for emergency thoracic endovascular aortic repair (TEVAR). Patient was intubated and sedated. Bilateral femoral access obtained and TERUMO (USA) 6F sheath used. JR 3.5/6F diagnostic catheter with TERUMO wire inserted in right femoral artery and pigtail catheter was inserted on the left femoral artery. Then SENTRANT Introducer Sheath (Medtronic, Ireland) 18 Fr inserted on the right femoral artery. TERUMO wire was exchanged with the stiff Back-up Meier guidewire (Boston Scientific,USA). Pigtail catheter was used to locate the level of dissection and aberrant right subclavian artery origin and determine the proximal landing zone. STENT VALIANT 26mm /152mm was deployed after the aberrant right subclavian artery. Pigtail catheter was used to locate origin of celiac artery to decide distal landing zone. Then, another STENT VALIANT 26mm/145mm extension was deployed until the level of T11 level just before the celiac artery origin at T12. Good results was seen. Right femoral access closed with 2 Perclose Proglide (Abbott, USA) closure device and left femoral access closed with Proglide. Total contrast used was 200 mls.
 RA, _video 1.mov
RA, _video 1.mov
RA, _VIdeo 2.mov
RA, _Video 3.mov
Case Summary
CT scan angiogram post 1 week and post 3 month showed no endoleak. Pre-procedure patient had fever and was treated with IV antibiotic to avoid infection of endograft. However all blood and urine cultures had no growth. One possible cause maybe that the fever was not due to infection but an inflammatory response to aortic dissection. Literature shows that fever can be present in acute aortic dissection with negative microbiological test. Hemoptysis develop due to formation of aortobronchial fistula between aortic dissection and the adjacent bronchus. TB screening was never positive in this patient. There was still hemoptysis post procedure but reduced and eventually resolved after few days.