
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-077
Intravascular Ultrasound Guided Controlled Retrograde Tracking After Failed Anterior Dissection Re-entry
By Kambis Mashayekhi, Faridun Rahimi, Najmiddin Makhkamov, Javokhir Anvarov
Presenter
Najmiddin Makhkamov
Authors
Kambis Mashayekhi1, Faridun Rahimi2, Najmiddin Makhkamov3, Javokhir Anvarov3
Affiliation
Heartcenter Lahr, Germany1, Doctor, Germany2, Fedorovich Klinikasi LLC, Uzbekistan3,
View Study Report
TCTAP C-077
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
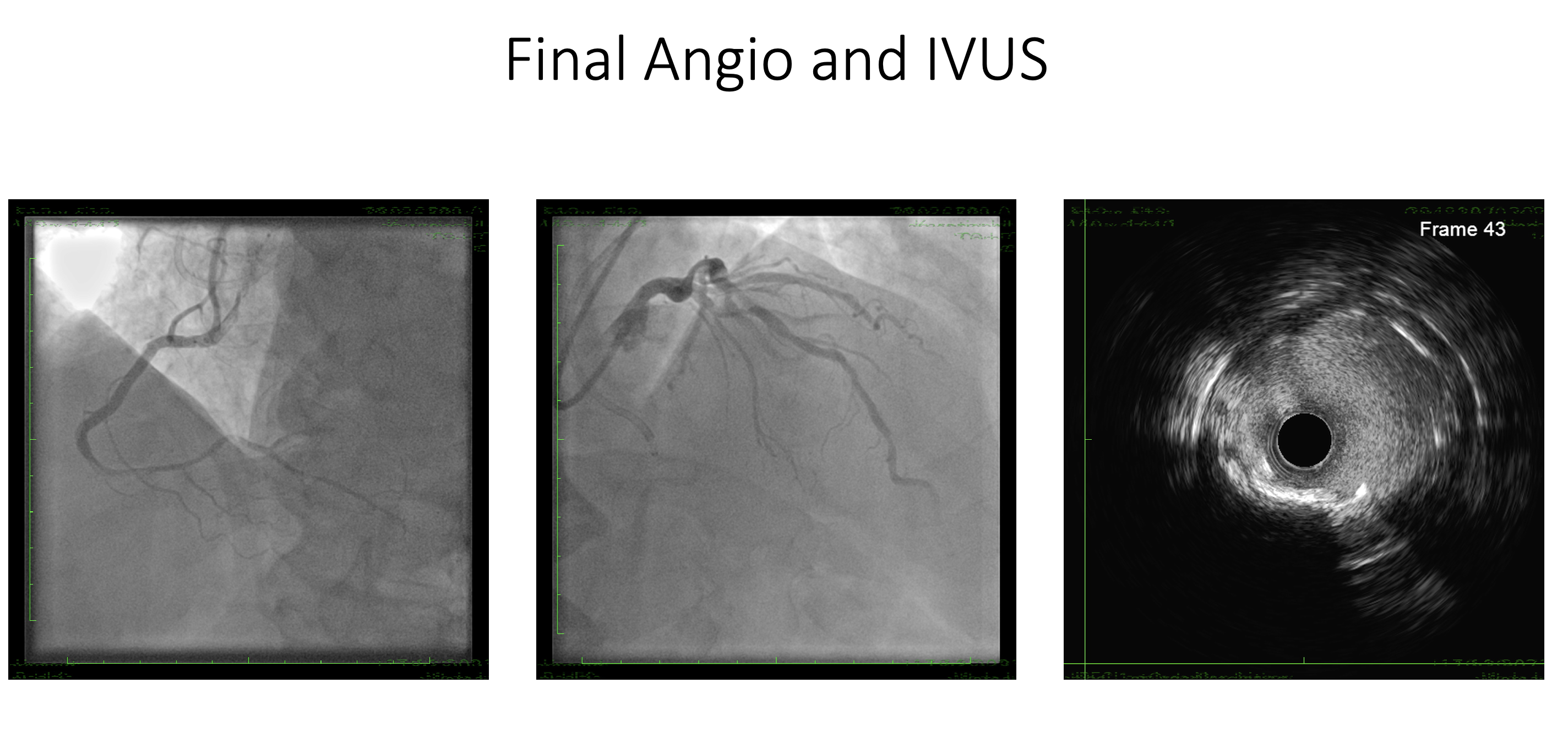
Intravascular Ultrasound Guided Controlled Retrograde Tracking After Failed Anterior Dissection Re-entry
Kambis Mashayekhi1, Faridun Rahimi2, Najmiddin Makhkamov3, Javokhir Anvarov3
Heartcenter Lahr, Germany1, Doctor, Germany2, Fedorovich Klinikasi LLC, Uzbekistan3,
Clinical Information
Patient initials or Identifier Number
S.H.
Relevant Clinical History and Physical Exam
Male 70 y.o.
Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
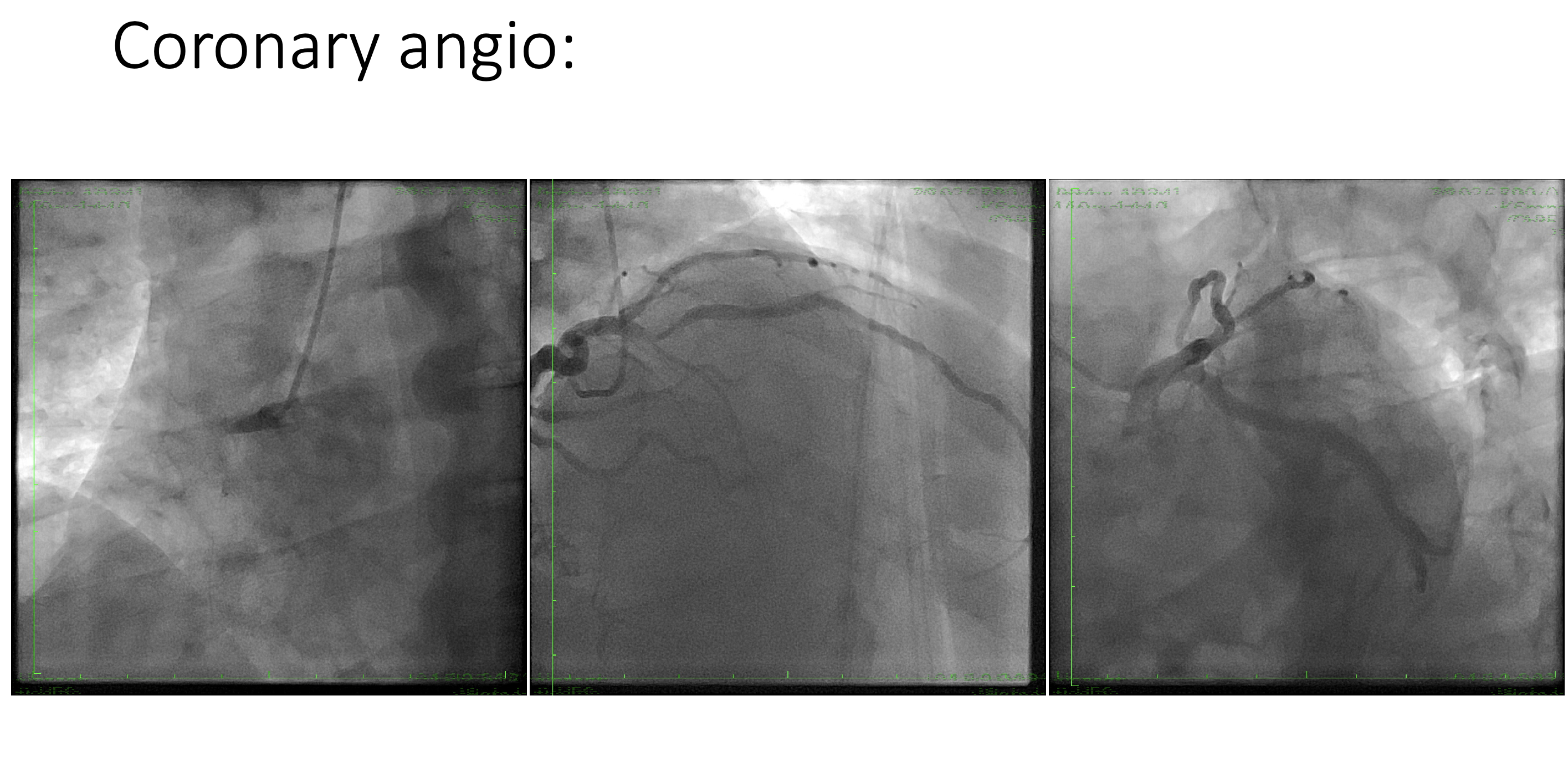
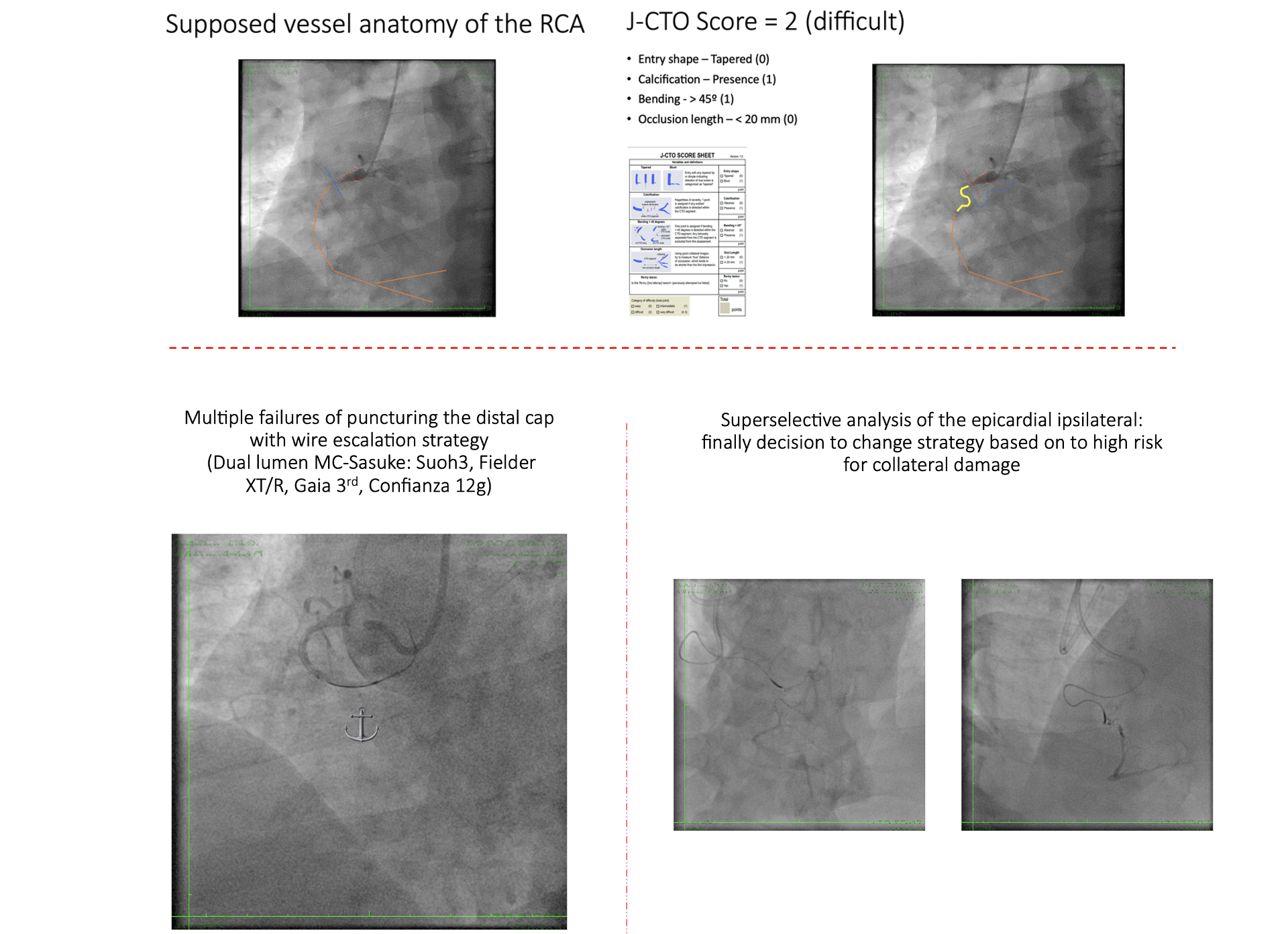
Coronary angio: 2 vessel disease. RCA - CTO from proximal segment. LAD - significant stenosis in middle part.
Interventional Management
Procedural Step
1. Bi-radial approach – 7F (RCA - AL1; XB 3.5 - LCA). Antegrade attempt: wire escalation from XT-R to Gaia 3rd
4. Failed IVUS guided antegrade puncture with Confianza Pro 12g, due to missing visualization of the distal vessel based on the calcified plaque.
with failure to re-enter.
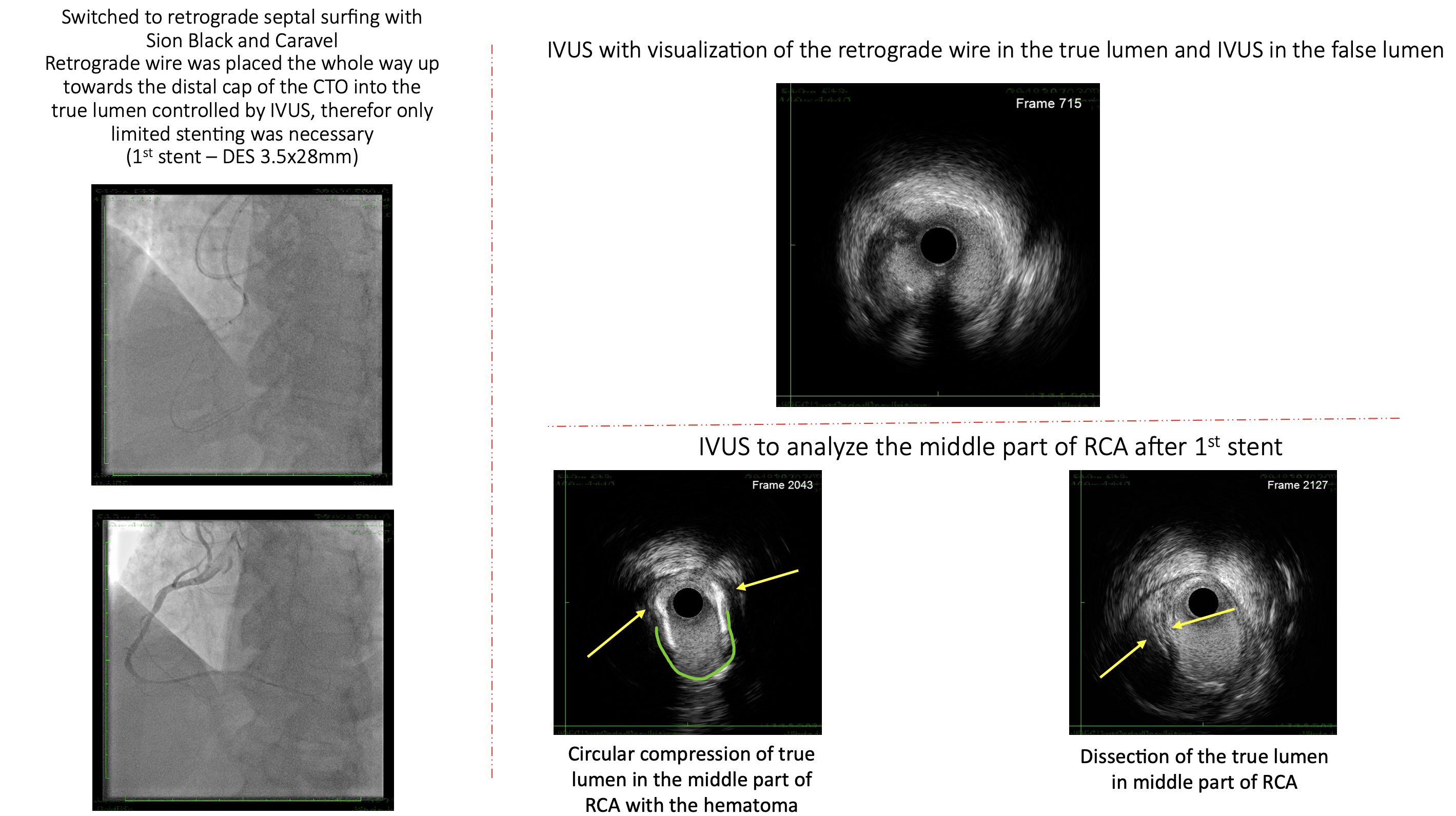
with IVUS controlled retrograde wire tracking.
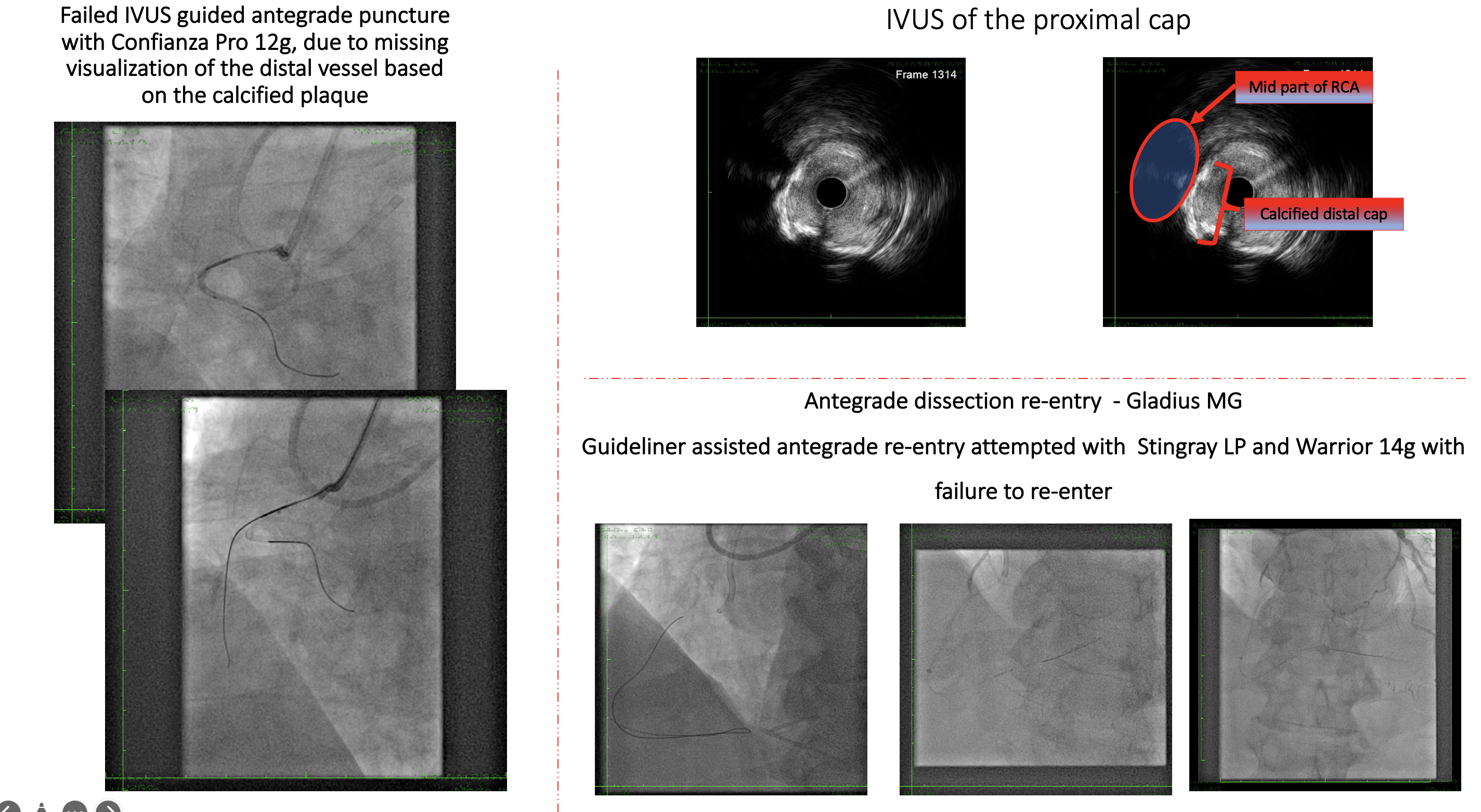
4. Failed IVUS guided antegrade puncture with Confianza Pro 12g, due to missing visualization of the distal vessel based on the calcified plaque.
with failure to re-enter.
with IVUS controlled retrograde wire tracking.
Case Summary
1) Never underestimate ”simple” CTO lesions.