
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-145
Successful Revascularization Case Using Trans-Radial Iliac Intervention With Direct Needle Crossing to the Calcified Plaque of CFA for Very Long Total Occlusion From CIA to CFA
By Shinya Ichihara, Naoki Hayakawa, Junji Kanda
Presenter
Shinya Ichihara
Authors
Shinya Ichihara1, Naoki Hayakawa1, Junji Kanda1
Affiliation
Asahi General Hospital, Japan1,
View Study Report
TCTAP C-145
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Successful Revascularization Case Using Trans-Radial Iliac Intervention With Direct Needle Crossing to the Calcified Plaque of CFA for Very Long Total Occlusion From CIA to CFA
Shinya Ichihara1, Naoki Hayakawa1, Junji Kanda1
Asahi General Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
F.I.
Relevant Clinical History and Physical Exam
A 63-year-old man with adiminished pulse in the dorsal foot artery was admitted to our hospital. He hadclaudication on the right limb. He had a past medical history of cerebralinfarction, and his regular medication was dual antiplatelet therapy withaspirin (100 mg) and clopidogrel (75 mg).
Relevant Test Results Prior to Catheterization
The ankle-brachial index (ABI) was 0.64 on the right side.Ultrasound examination and contrast-enhanced computed tomography (CT) revealed severe calcification and suspected occlusion from the right iliac artery to the common femoral artery (CFA).

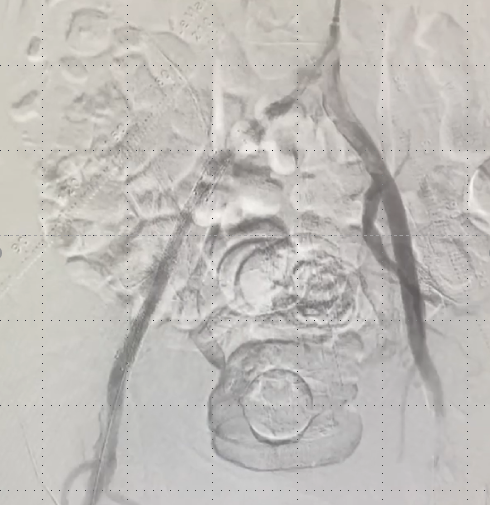
Relevant Catheterization Findings
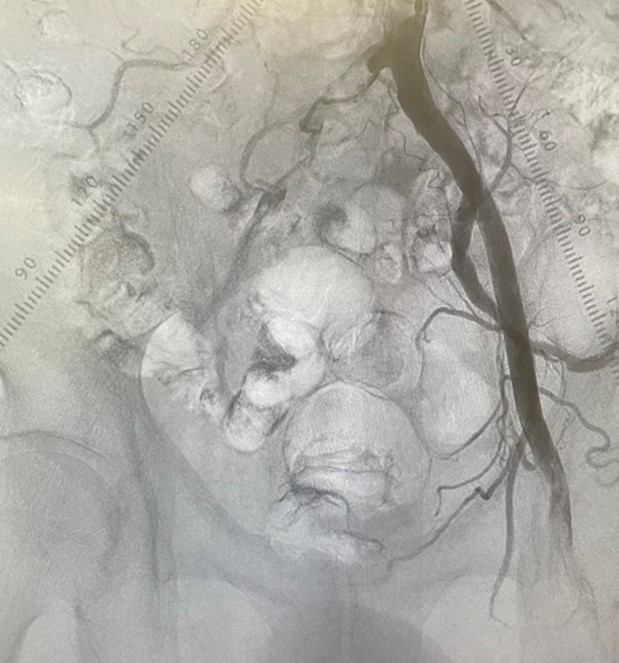
We inserted the 5-6Fr Glidessheath slender into the left radial artery and performed angiography. As expected from the preliminary examination, the control angiography showed total occlusion from the right common iliac artery (CIA) to the CFA.
Interventional Management
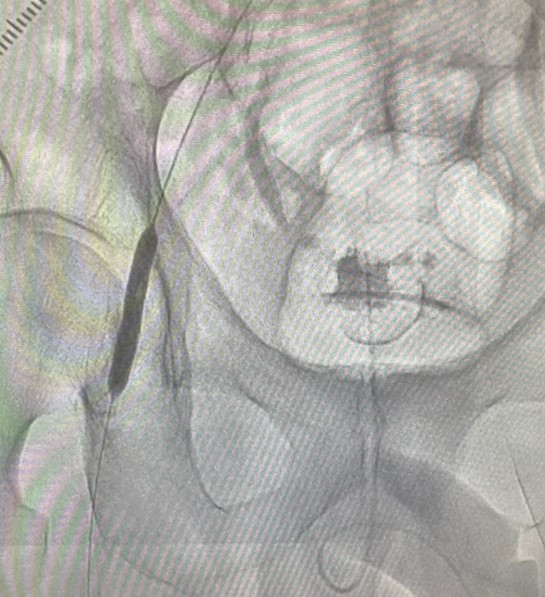
Procedural Step
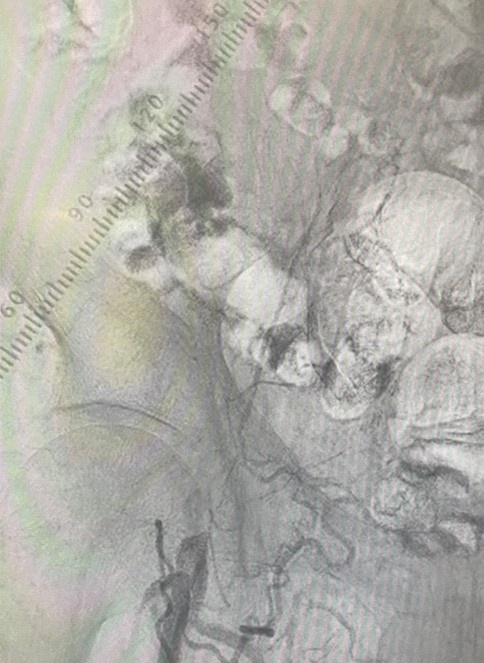
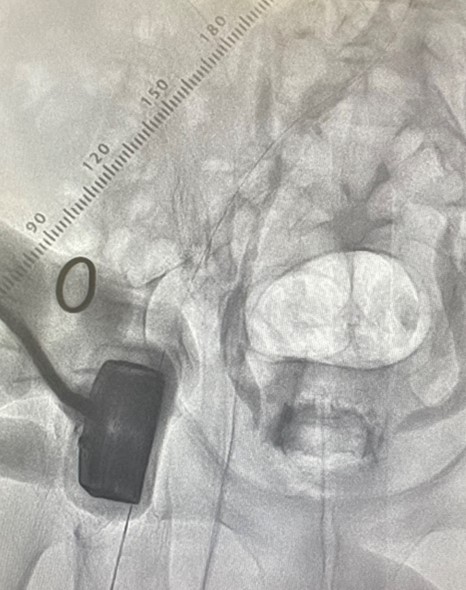
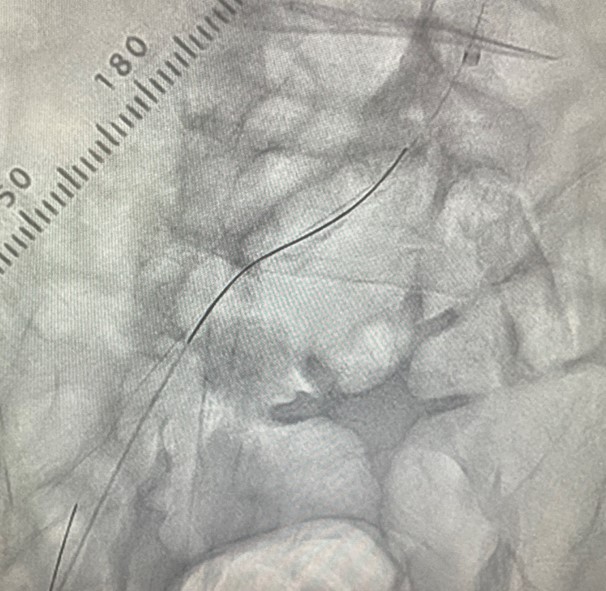
We inserted 6Fr guiding sheath from left radial artery.Before the wiring, we performed the CTfusion three-dimensional roadmap (CTf3D-RM) technique,which is our original technique of multi-modality fusion of preprocedural CT and angiography. With the guidance of CTf3D-RM, a 0.014-inch Gladius MG guidewire and Caravel microcatheter was advanced into EIA, but antegrade crossing was difficult. Therefore,we decided to perform the retrograde approach.However, there was big problem of severe calcified plaque in the CFA. So we performed retrograde direct metal needle puncture to calcified plaque from CFA distal lumen. 21-G needle with bending of its tips could be advanced in the center of calcified plaque, then a Gladius guidewire was advanced into the EIA. Next, a Corsair Armetmicrocatheter was introduced as a sheath-less technique. We performed IVUS guided wiring with antegrade IVUSand retrograde Halberd 0.014-inch guidewire. After that, we could achieve the wire-externalization, and guidewire was all intraplaque route. After the 4.0mm balloon dilation, we advanced the Gladius wire to popliteal artery from antegradely. We dilated 6.0mmhigh-pressure balloon for CFA calcified lesion with intravascular hemostasis of retrograde puncture site.IVUS showed sufficient lumen area in the CFA. Finally,we deployed 3 nitinol stents for EIA distal to CIA ostium, and we dilated Lutonix DCB for CFA. Final angiography was very well and he could go back to bedroom on foot.
Case Summary
We could succeed very tough case of long CTO from CIA to CFA with heavy calcification less invasively. The combination ofCTf3D-RM, direct needle crossing to calcified CFA, IVUS guided wiring, and trans radial EVT were feasible strategy for complex aortoiliac case with minimal invasiveness.