
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-049
Stent Size Matters
By Khin Maung Zan Mohd Saad Jalaluddin, Yee Sin Tey, Kumara Gurupparan Ganesan
Presenter
Khin Maung Zan Mohd Saad Jalaluddin
Authors
Khin Maung Zan Mohd Saad Jalaluddin1, Yee Sin Tey2, Kumara Gurupparan Ganesan2
Affiliation
Hospital Pusrawi, Malaysia1, National Heart Institute, Malaysia2,
View Study Report
TCTAP C-049
CORONARY - Bifurcation/Left Main Diseases and Intervention
Stent Size Matters
Khin Maung Zan Mohd Saad Jalaluddin1, Yee Sin Tey2, Kumara Gurupparan Ganesan2
Hospital Pusrawi, Malaysia1, National Heart Institute, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Mr. SAH
Relevant Clinical History and Physical Exam
71 year old gentleman with underlying hypertension, dyslipidemia and coronary artery disease with previous angioplasty to left anterior descending artery (LAD) with Drug Eluting Stent (DES) 2.75 x 15 mm. He presented with recurrent unstable angina. He is a non-smoker and there was no family history of coronary artery disease. Clinical examinations were unremarkable and there was no evidence of heart failure.
 TCTAP 2022 VIDEO 1.mp4
TCTAP 2022 VIDEO 1.mp4
TCTAP 2022 VIDEO 2.mp4
TCTAP 2022 VIDEO 3.mp4
Relevant Test Results Prior to Catheterization
Electrocardiogram (ECG) showed no significant ST-T wave changes. Echocardiogram showed left ventricular ejection fraction (LVEF) of 50% with regional wall motion abnormalities at anterior wall. His eGFR was normal. Total cholestrol was 5.2 mmol/L with LDL-c of 2.1 mmol/L and HbA1c of 5.8%.
TCTAP 2022 VIDEO 7.mp4
Relevant Catheterization Findings
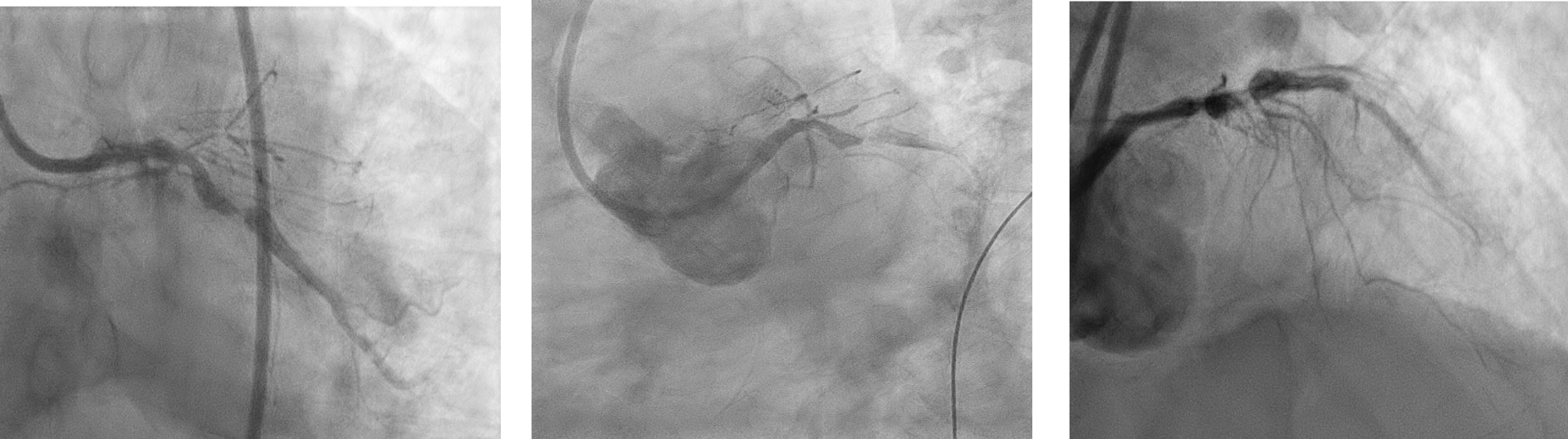
Coronary angiogram showed severe stenosis of Left Main Stem (LMS), tight stenosis of proximal Left Circumflex artery (LCx) with slow flow and Chronic total occlusion (CTO) from ostial Left Anterior Descending (LAD) artery and mild disease of Right Coronary Artery (RCA) with good retrograde flow to LAD. He was offered option of Coronary Artery Bypass Graft (CABG) but refused and opted for complex coronary intervention.
Interventional Management
Procedural Step
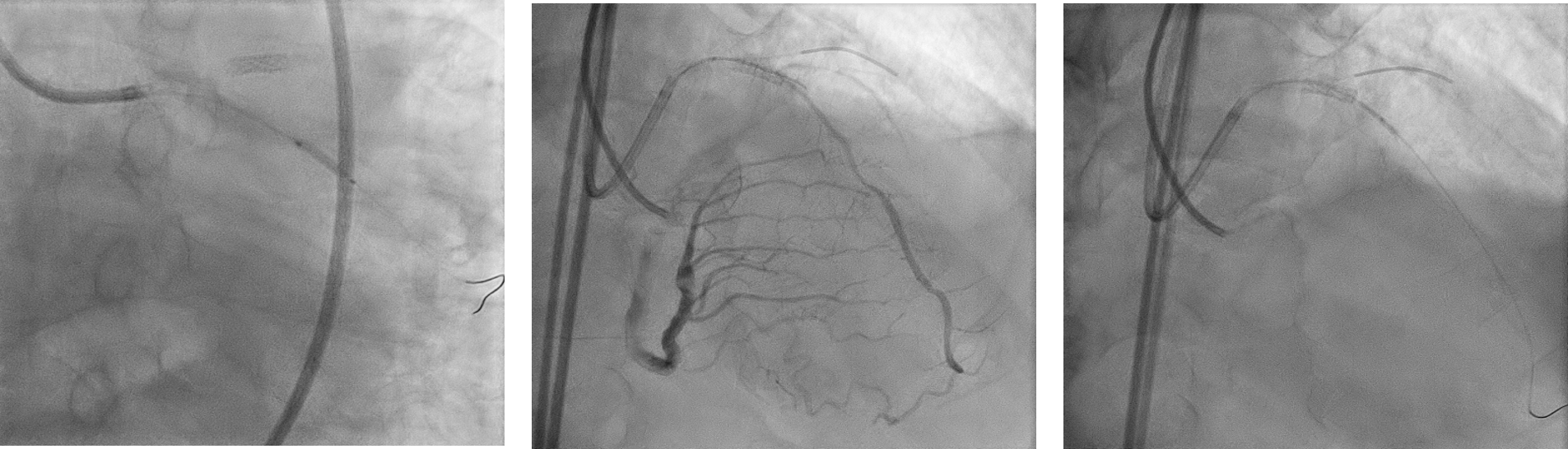
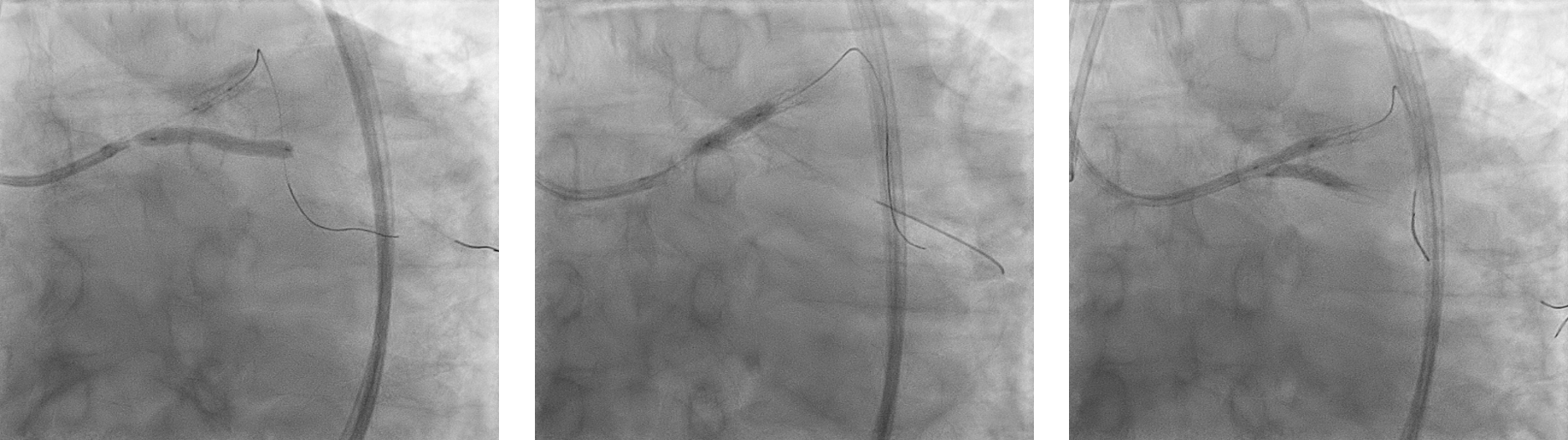
We proceeded with complex coronary intervention to LM-LAD-LCX with bifurcation double kissing (DK) crush strategy. Initially, predilated tight proximal LCX lesion with sapphire II pro 2.0x12 mm to establish good blood flow to LCX. Attempted to cross CTO LAD with Fielder XT and Gaia second wire with Finecross was unsuccessful as wire was subintimal. Finally crossed CTO lesion with CROSS-IT 200XT wire and exchanged to runthrough floppy wire. Sequential predilatation was done with SC 1.5X12 mm, SC 2.5X15 mm and scoreflex NC 3.0x15 mm balloons.
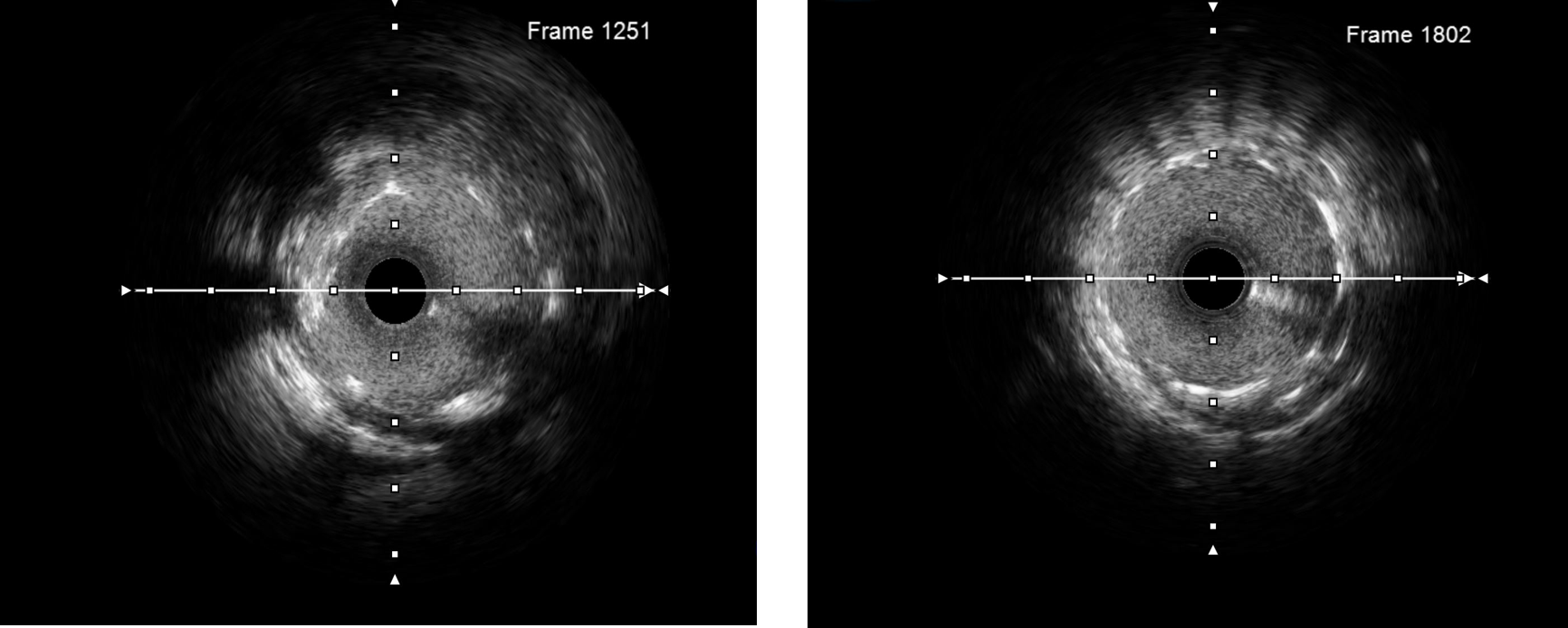
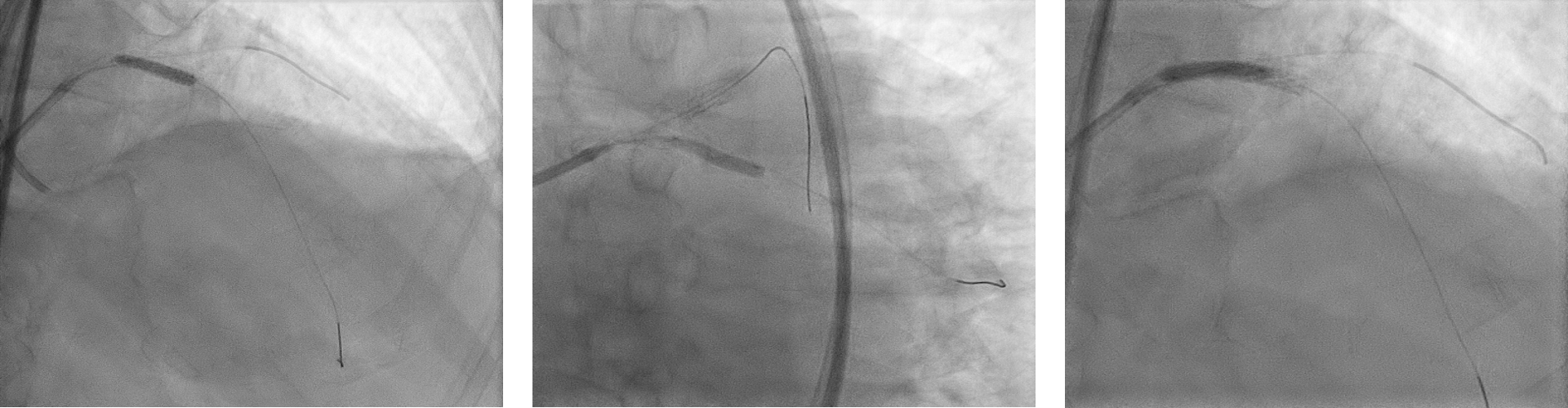
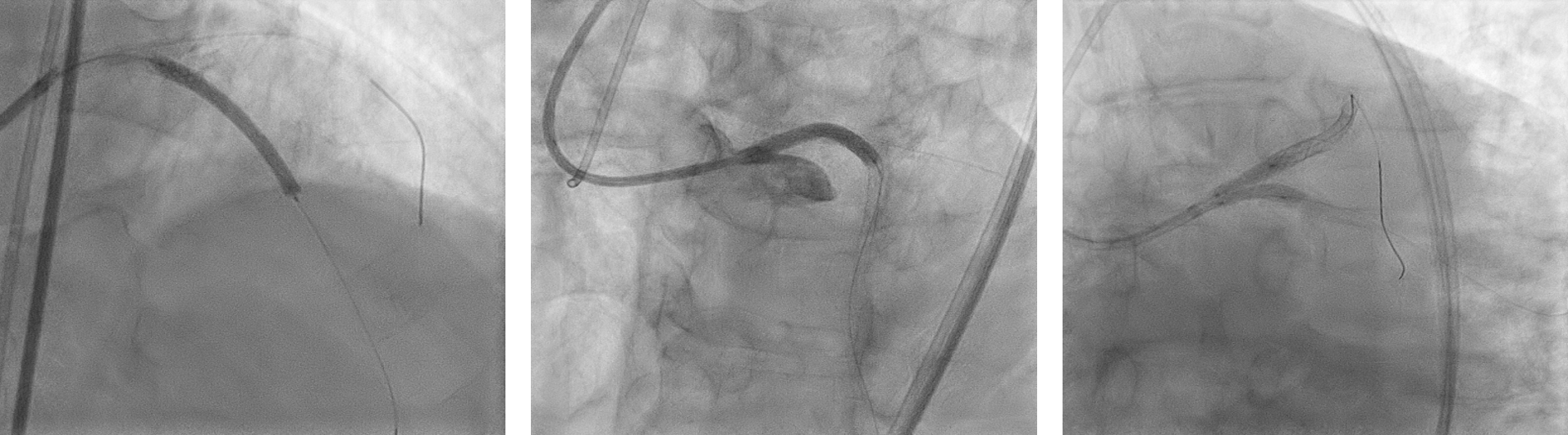
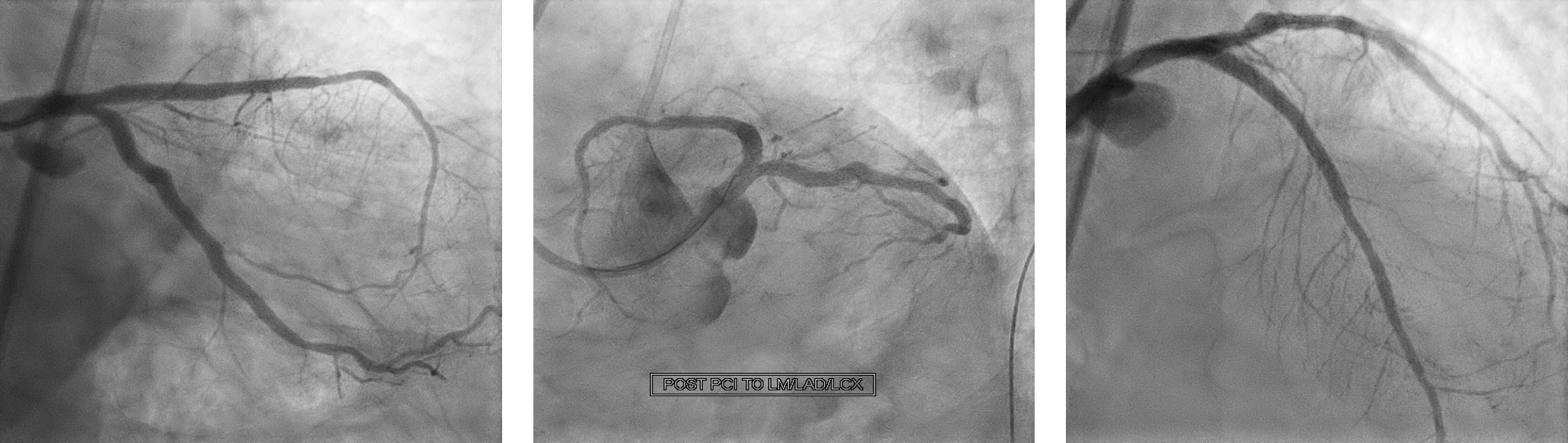
Intravascular Ultrasound (IVUS) was done and noted previous LAD stent was undersized with 2.75 mm diameter stent in a 3.5-4.0 mm diameter vessel. This could be the cause of CTO ostial LAD. We did further predilatation with scoreflex NC 3.5x15 mm to both LAD and LCX. Stented LCX with Resolute Onyx 3.5x22 mm and crushed with NC emerge 3.5x15 mm. Rewired to LCX and first kissing was done with 2 NC emerge 3.5x15 mm. Stented mid LAD with Resolute Onyx 3.0x38 mm and LM-LAD with Resolute Onyx 3.5x34 mm. Proximal Optimization (POT) to LM with NC emerge 4.0x8 mm and rewired LCX. Postdilated LAD and LCX stents with NC emerge 3.5x15 mm. Second kissing was done with 2 NC emerge 3.5x15 mm and final POT to LM with NC emerge 4.0x8 mm at 18 atm. noted another lesion at distal LCX and stented with Resolute ONYX 2.75x26mm. Post procedure IVUS run showed stents were well apposed. Final result was good and patient was stable throughout the procedure.
TCTAP 2022 VIDEO 8.mp4
TCTAP 2022 VIDEO 4.mp4
Intravascular Ultrasound (IVUS) was done and noted previous LAD stent was undersized with 2.75 mm diameter stent in a 3.5-4.0 mm diameter vessel. This could be the cause of CTO ostial LAD. We did further predilatation with scoreflex NC 3.5x15 mm to both LAD and LCX. Stented LCX with Resolute Onyx 3.5x22 mm and crushed with NC emerge 3.5x15 mm. Rewired to LCX and first kissing was done with 2 NC emerge 3.5x15 mm. Stented mid LAD with Resolute Onyx 3.0x38 mm and LM-LAD with Resolute Onyx 3.5x34 mm. Proximal Optimization (POT) to LM with NC emerge 4.0x8 mm and rewired LCX. Postdilated LAD and LCX stents with NC emerge 3.5x15 mm. Second kissing was done with 2 NC emerge 3.5x15 mm and final POT to LM with NC emerge 4.0x8 mm at 18 atm. noted another lesion at distal LCX and stented with Resolute ONYX 2.75x26mm. Post procedure IVUS run showed stents were well apposed. Final result was good and patient was stable throughout the procedure.
Case Summary
In conclusion, this is a case of successful revascularization to LM-CTO LAD-LCX with DK crush strategy. This case demonstrates that proper stent size should be used to improve procedural outcome and future events. Initial undersized stent could be the cause of chronic total occlusion that eventually caused recurrent unstable angina in this case. Intravascular imaging is crucial to evaluate vessels sizes and characteristics, proper stent selection, assess stents apposition especially when we are dealing with Left Main, CTOs or other complex coronary interventions including long diffuse disease. Patient was well and asymptomatic during 6 months post procedure follow up and LVEF remains 50-55%.