
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-109
Severe Iatrogenic Aortic Dissection Resolved in Five Days After Aorto-Ostial Stenting
By Yi Lin Tsai, Chin Chin Chang, Tse-Min Lu, Ju-Pin Pan
Presenter
Yi Lin Tsai
Authors
Yi Lin Tsai1, Chin Chin Chang1, Tse-Min Lu1, Ju-Pin Pan1
Affiliation
Taipei Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-109
CORONARY - Complications
Severe Iatrogenic Aortic Dissection Resolved in Five Days After Aorto-Ostial Stenting
Yi Lin Tsai1, Chin Chin Chang1, Tse-Min Lu1, Ju-Pin Pan1
Taipei Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Chai
Relevant Clinical History and Physical Exam
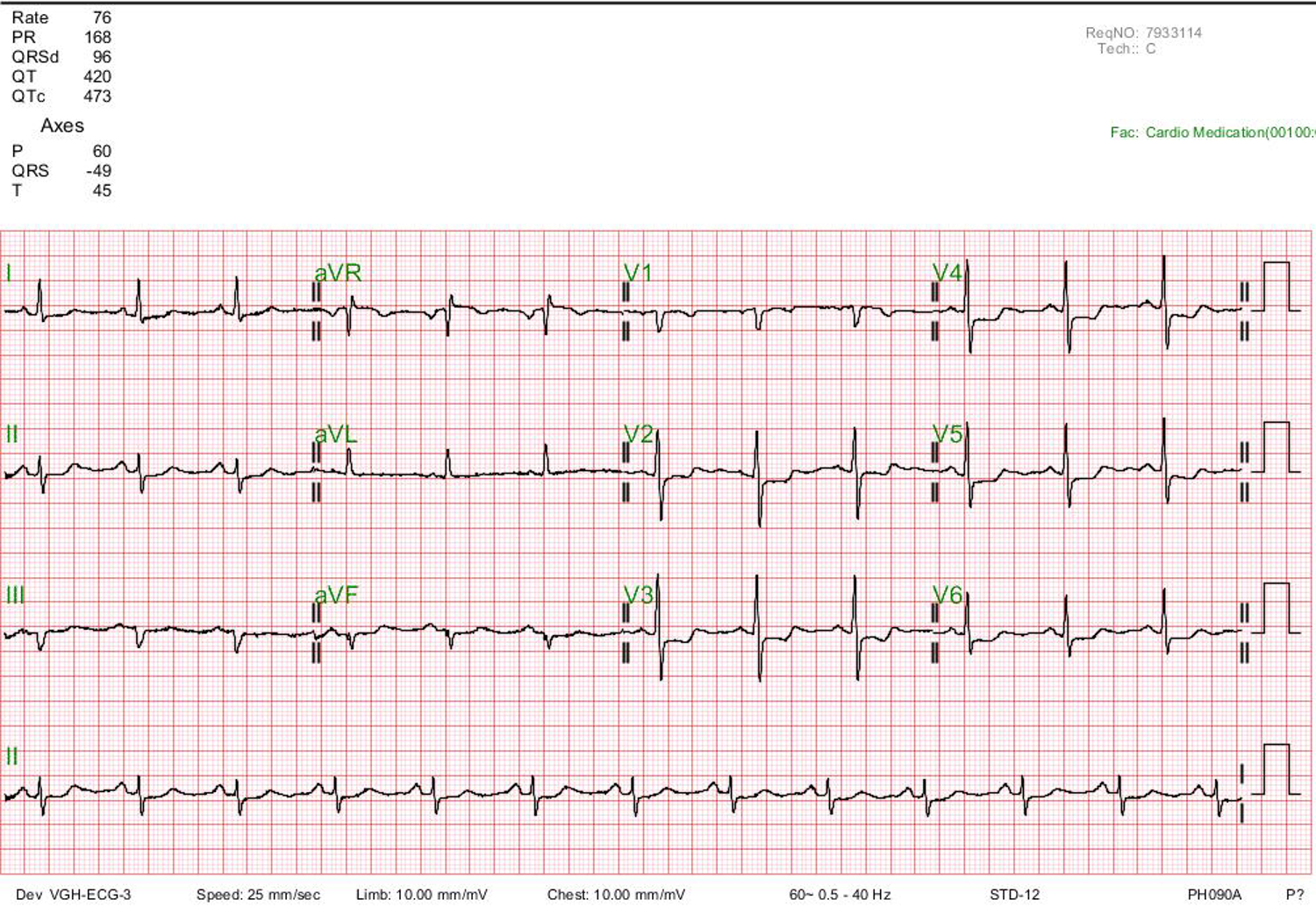
A 65-year-old woman who had a history of hypertension and dyslipidemia under medical therapy came to the clinic due to effort-related chest tightness and dyspnea on exertion for months. At present, her hemodynamics were stable and no remarkable findings from a physical examination. The 12-lead electrocardiogram revealed diffuse precordial leads (V2~V6) and inferolateral leads (I, II) ST-segment depression. The initial laboratory tests were normal, with no elevation of the cardiac enzyme.
Relevant Test Results Prior to Catheterization
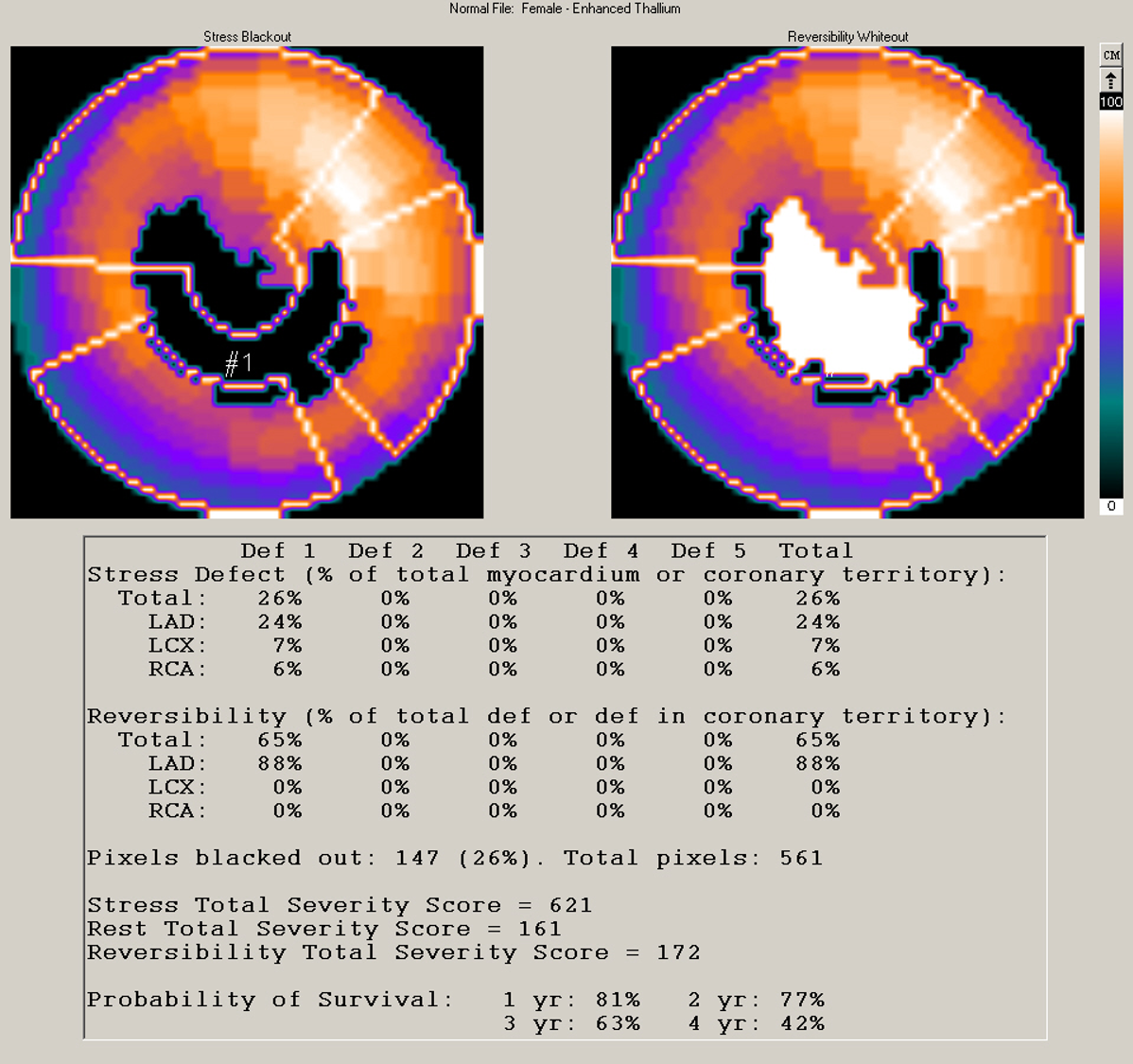
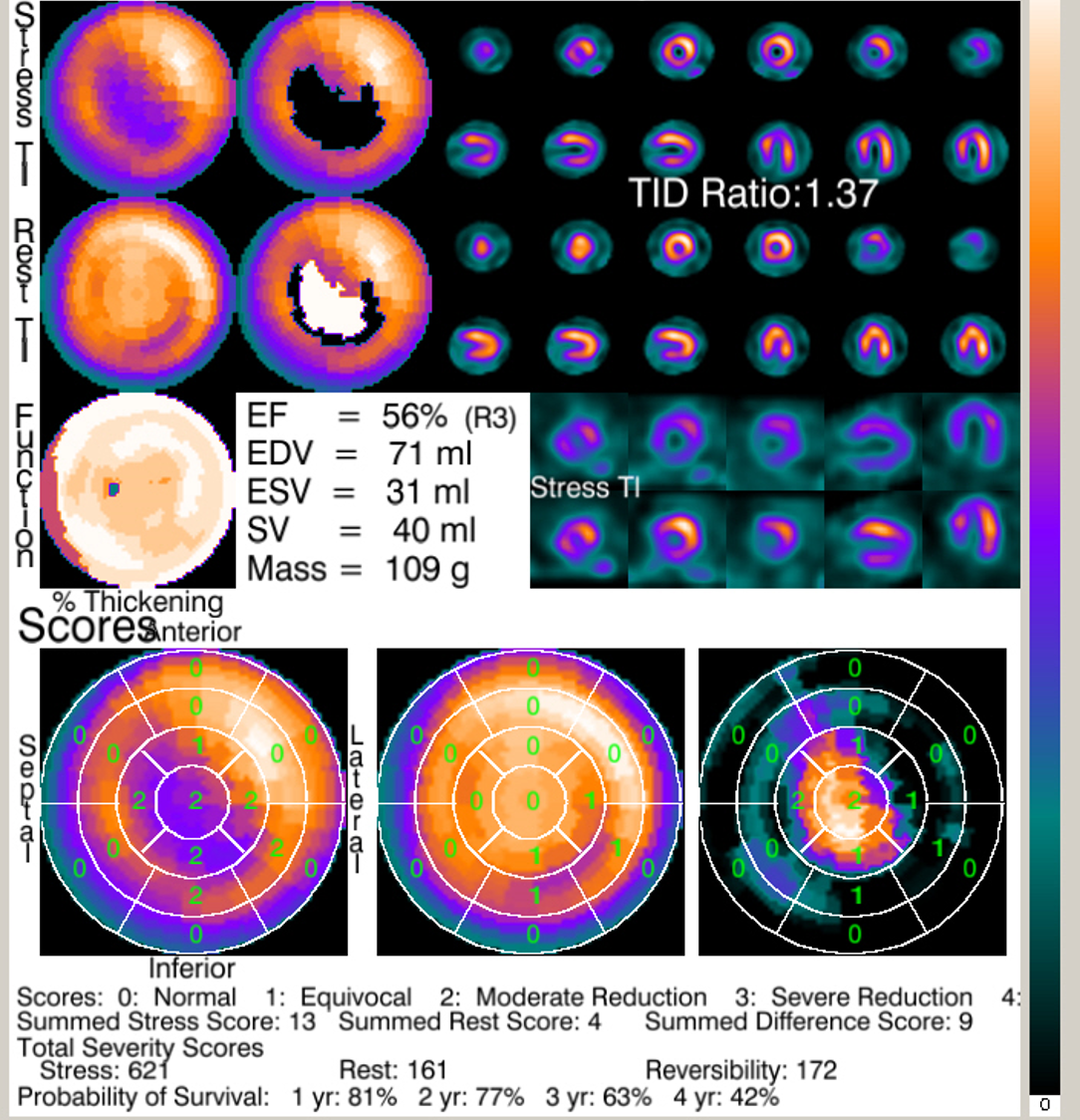
Her thallium scan revealed a large area of stress defect over the inferior and apical wall with a total of 26% ischemic burden and high reversibility. The transient ischemic dilatation ratio was 1.37.
Relevant Catheterization Findings
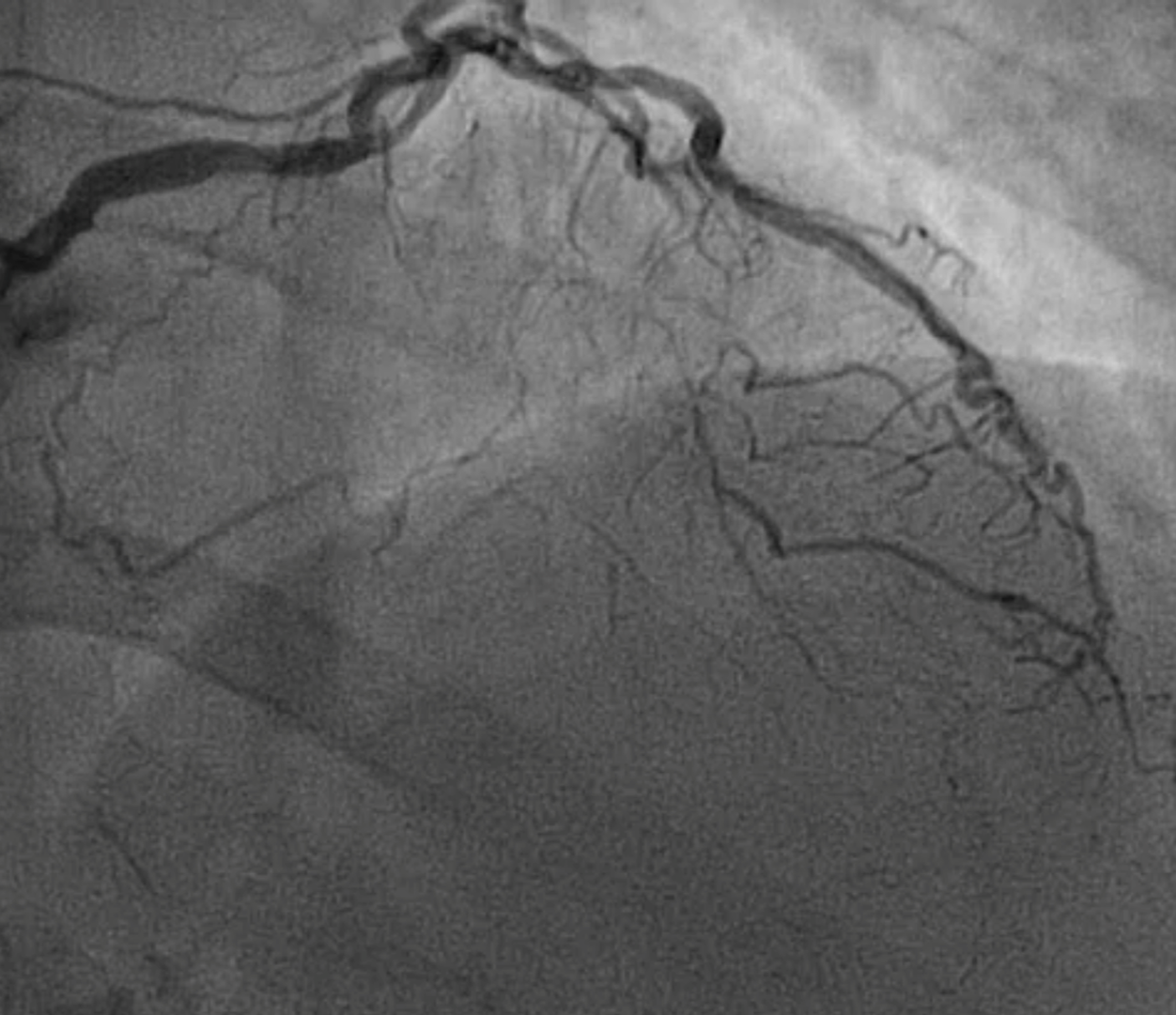
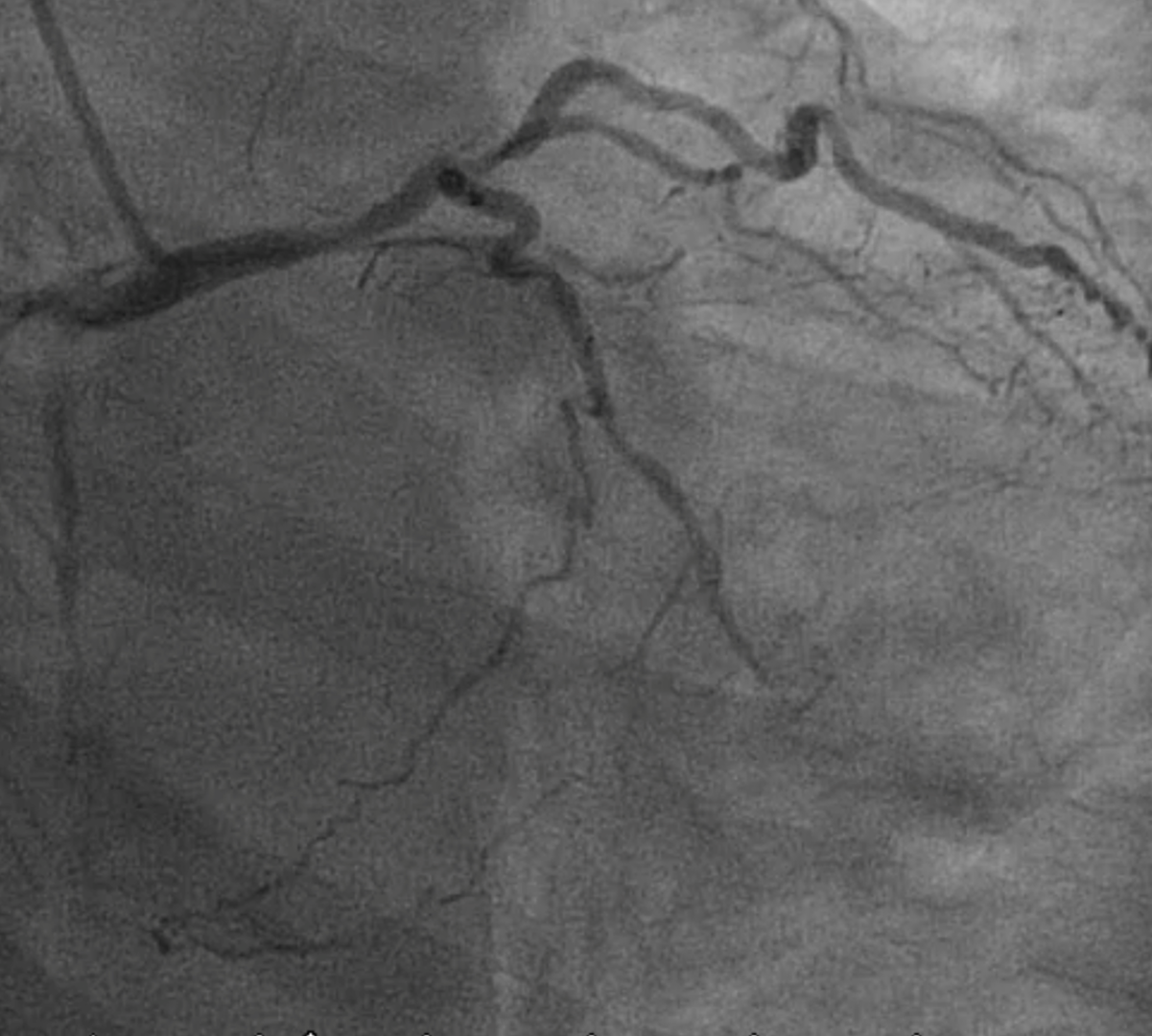
The coronary artery angiogram (CAG) revealed dominant right coronary artery (RCA) with ostium critical stenosis related to calcified plaque. The distal left main (LM) shaft also had moderate disease and the left anterior descending artery (LAD) was chronic total occlusion (CTO) from the ostium with a blunt end. The collateral channels of LAD mainly came from the RCA posterior descending artery.

Interventional Management
Procedural Step
Considering the LAD was total occluded from the ostium with blunt end, retrograde approach might be required for LAD recanalization. Therefore, we revascularized RCA with ostial stenting by drug eluting stent (DES). After RCA PCI, her symptoms improved but still complained effort related chest tightness. The LAD CTO PCI was conducted after one month. The LAD CTO was recanalized by antegrade wire escalation technique after intra-vascular ultrasound (IVUS) located the CTO proximal cap. After IVUS evaluation the disease segment extended from LAD to LM shaft, 2 DES were deployed from LAD middle segment to LM proximal with provisional stenting. After final proximal optimizing technique to fix the LM stent, the angiogram revealed LM and LAD TIMI 3 antegrade flow. However, a dissection flap near LM stent with retrograde iatrogenic aortic dissection was noticed. The contrast medium extended beyond the coronary cuspid up to the ascending aorta.In the meantime, the patient complained acute and sharp chest pain. IVUS image confirmed the proximal stent edge dissection and another DES was deployed over LM ostium to seal the flap. Final angiogram confirmed no more progression of retrograde aortic dissection and the severity of dye staining was reduced.he initial computed tomography angiogram (CTA) revealed severe iatrogenic aortic dissection, after 5 days of medical treatment, the follow-up CTA showing the severe iatrogenic aortic dissection was nearly resolved.
 Vedio 1.mp4
Vedio 1.mp4
Vedio 2.mp4
Vedio 3.mp4
Vedio 4.mp4
Vedio 5.mp4
Vedio 6.mp4
Vedio 7.mp4
Vedio 8.mp4
Case Summary
Stent edge dissection is one of the complications during PCI and may deteriorate after forceful contrast injection. In our case, unnoticed LM stent proximal stent edge dissection with severe retrograde aortic dissection happened during taking the post stenting angiogram. In our case report, after sealing the LM dissection flap by IVUS-guided DES implantation, the severe iatrogenic aortic dissection could be resolved rapidly after five days concomitant with medical therapy.