
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-168
Structural Interventional Solution When Coronary Revascularization and Optimal Medical Therapy Are Not Enough
By Farhat Fouladvand, Gaetano Di Palma, Elisabetta Iardino, Bernardo Cortese
Presenter
Gaetano Di Palma
Authors
Farhat Fouladvand1, Gaetano Di Palma1, Elisabetta Iardino2, Bernardo Cortese1
Affiliation
Clinica San Carlo, Italy1, Ospedale Bolognini, Italy2,
View Study Report
TCTAP C-168
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Structural Interventional Solution When Coronary Revascularization and Optimal Medical Therapy Are Not Enough
Farhat Fouladvand1, Gaetano Di Palma1, Elisabetta Iardino2, Bernardo Cortese1
Clinica San Carlo, Italy1, Ospedale Bolognini, Italy2,
Clinical Information
Patient initials or Identifier Number
DS 22/01/1983
Relevant Clinical History and Physical Exam
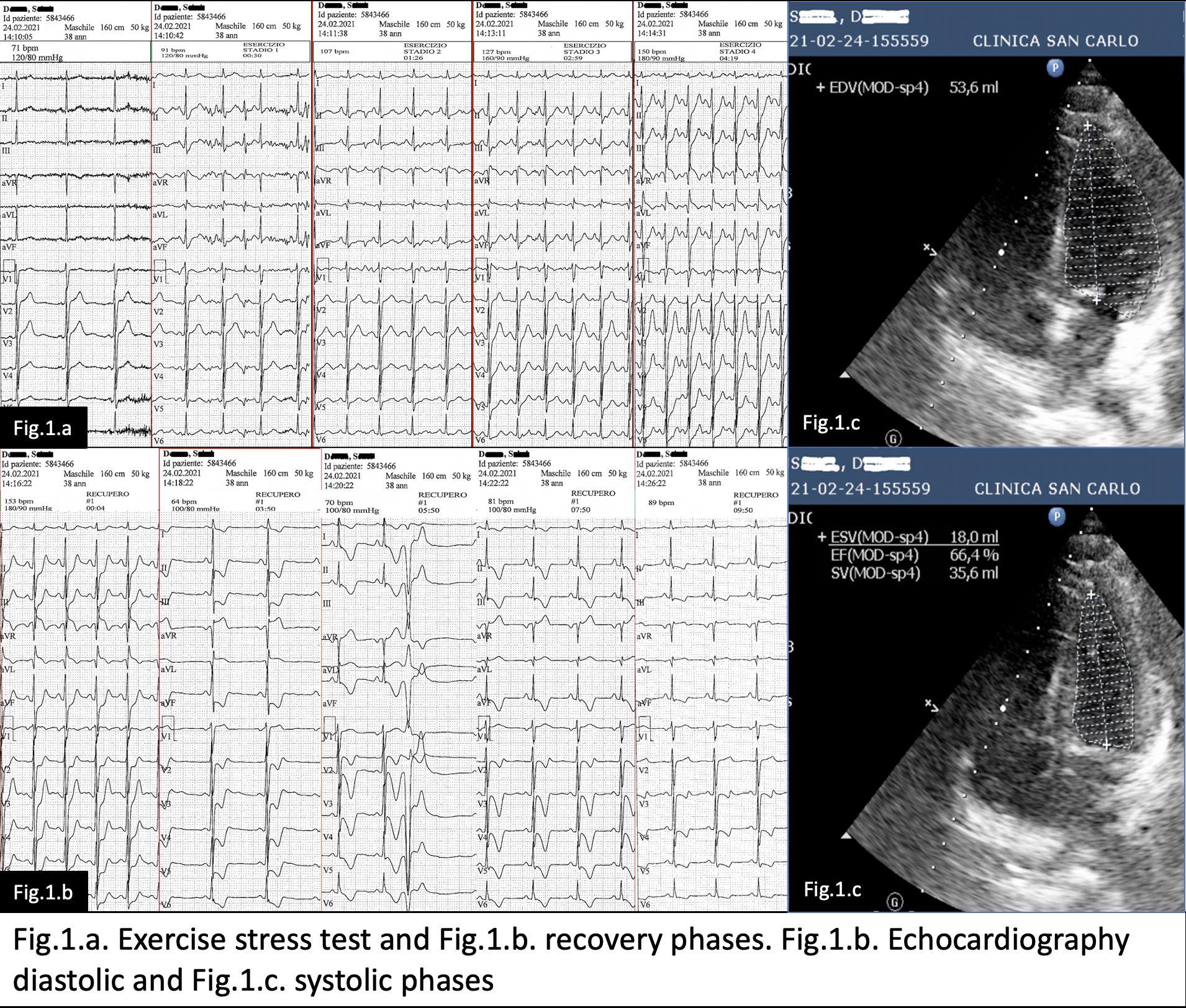
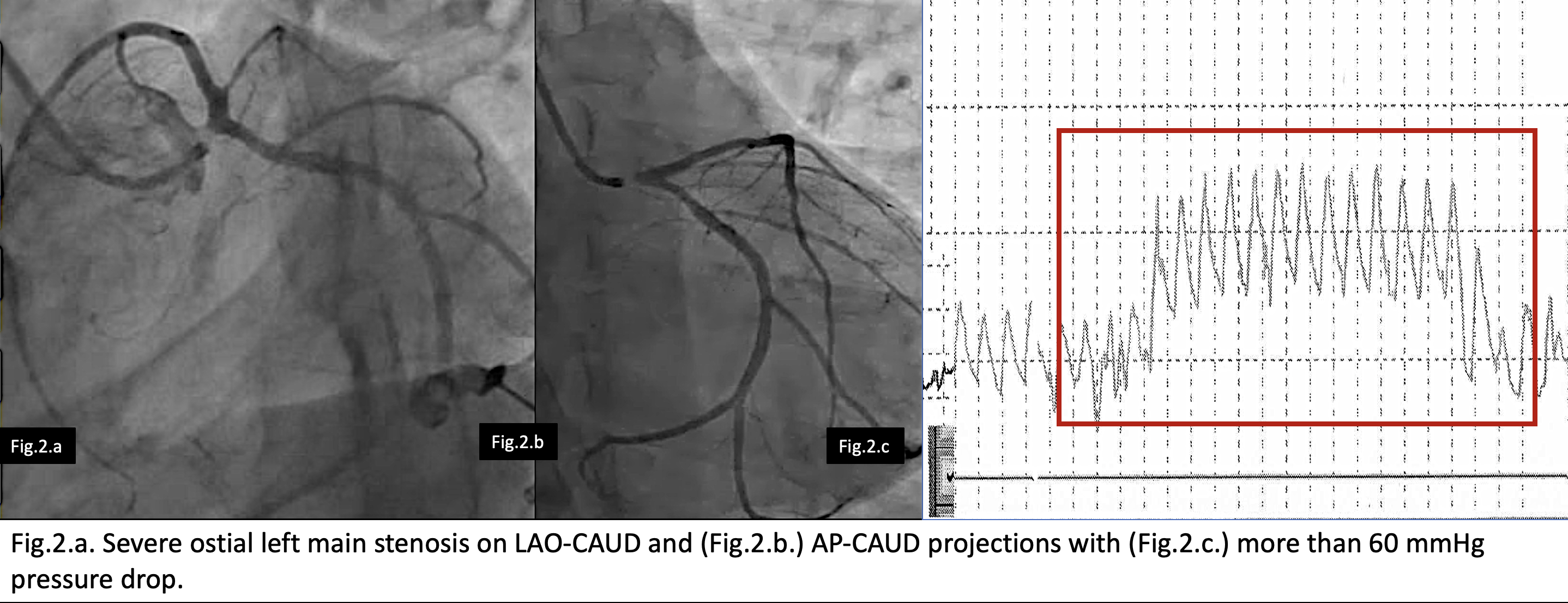
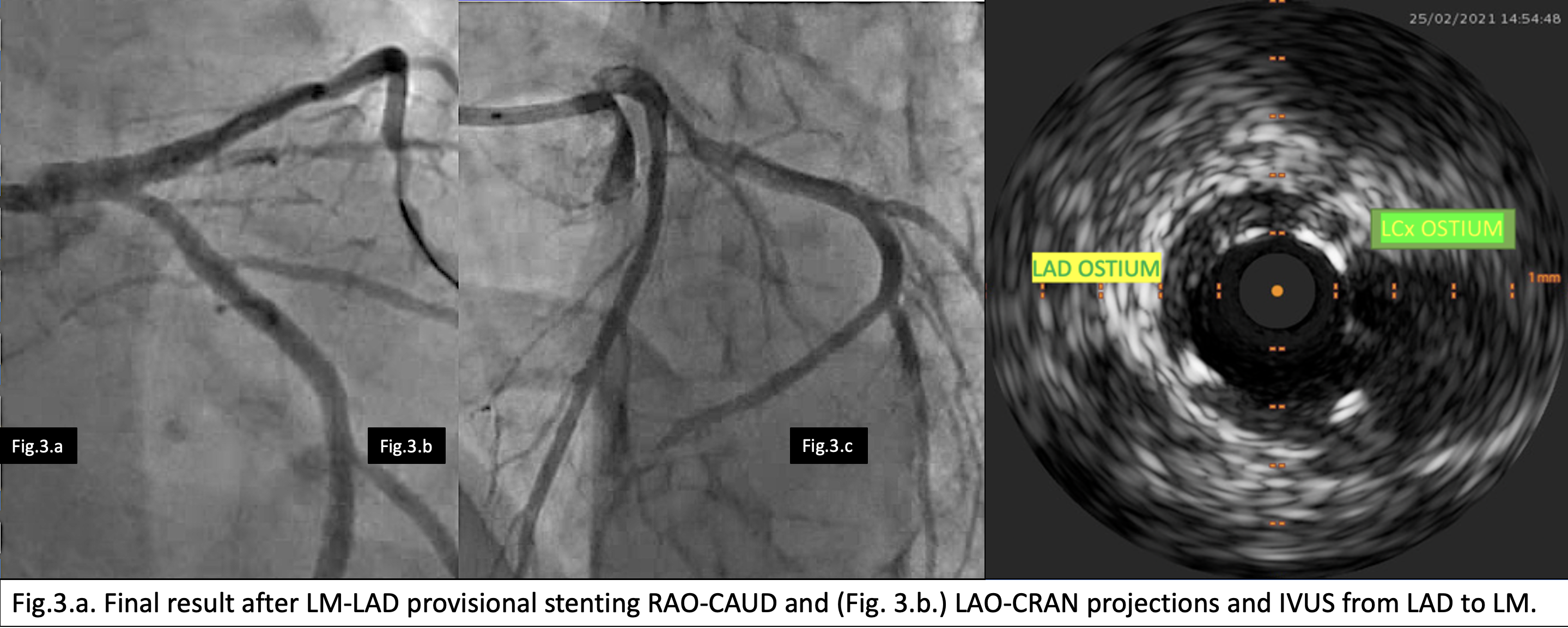
We describe a case of a 38 y male with diabetes and effort angina (CCS 3) that was recovered immediately after severely positive exercise test (Fig.1.a-b.). His echocardiography shoed no wall motion abnormalities and normal ejection fraction (Fig.1.b-c.). Angiography shoed severe ostial left main stenosis (Fig.2.) that was treated with provisional LM-LAD stenting with good angiographic (Fig.3.a-b) and IVUS (Fig.3.c.) result. After 3 months he came back to us for persistence of effort angina.
Relevant Test Results Prior to Catheterization
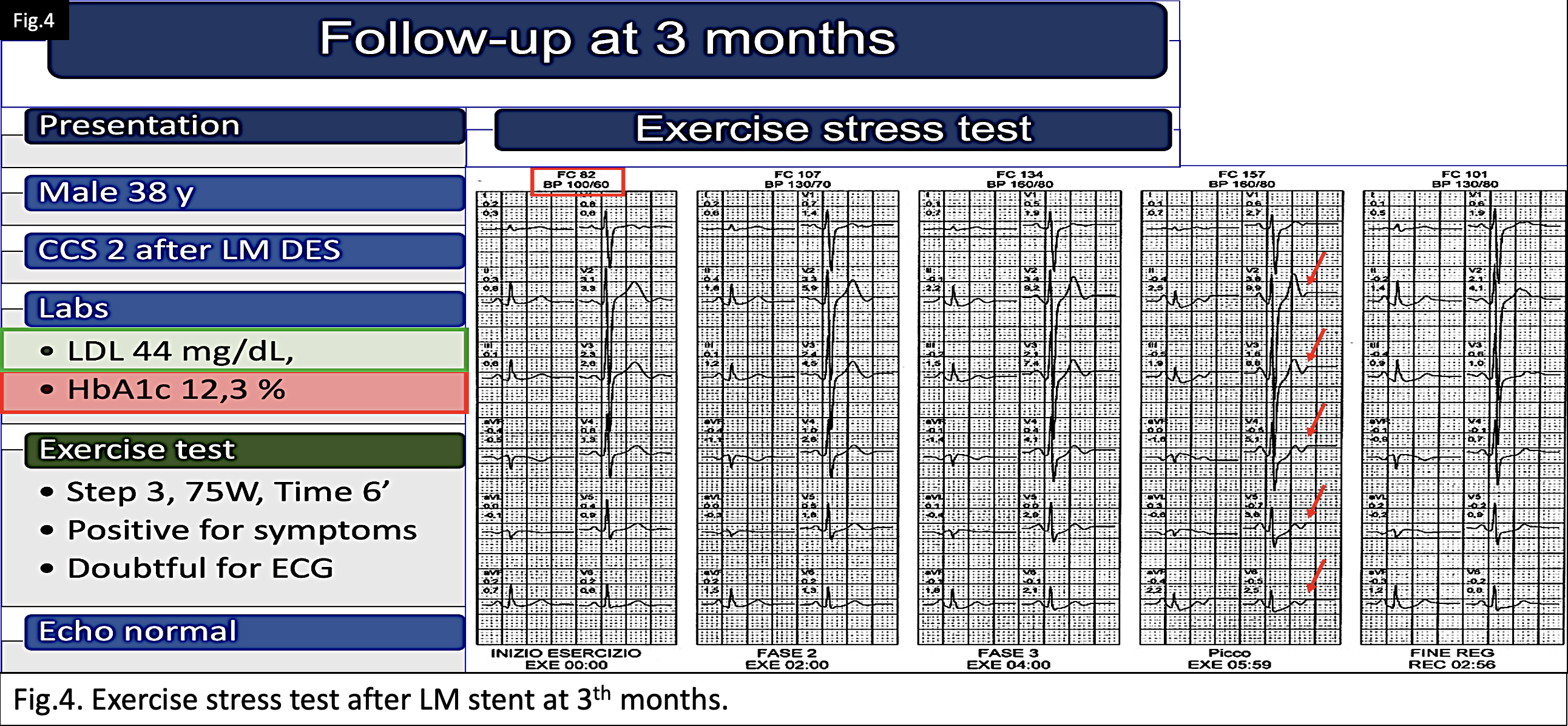
The patient was hypotensive and with bad compliance to the medical therapy, so there was no more option for optimization of the medical treatment. Echocardiography was again normal. We performed the same type of exercise test that was interrupted at 6th minute for chest pain with doubtful changes in the ECG. The patient had optimal lipids level but still desired optimization of blood sugar (Fig.4). He was recovered for coronary angiography.
Relevant Catheterization Findings
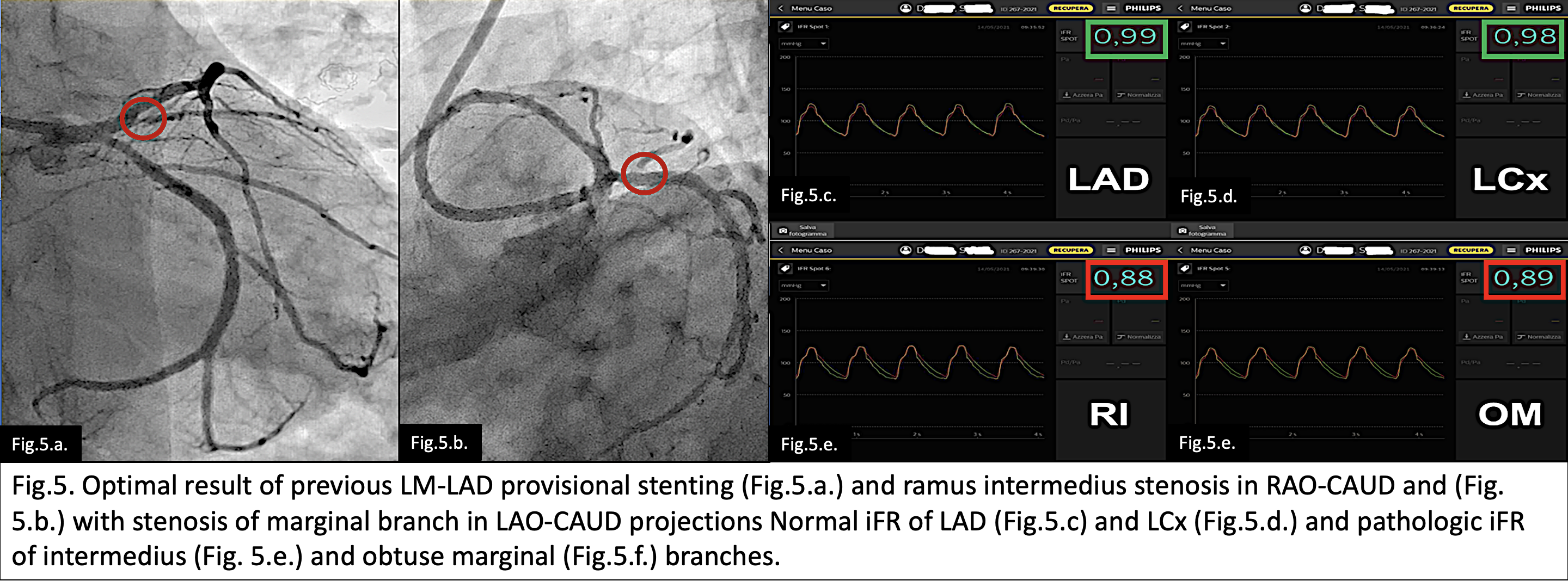
Angiography shoed good result of LM stent (Fig.5.a-b) with normal instantaneous free wave ratio (iFR) on LAD iFR = 0,99 and LCx iFR = 0,98 (Fig. c-d), but pathologic values on small (<1,5 mm) diffusely diseased RI iFR = 0,89 and marginal branches (OM iFR = 0,88) (Fig.5.e-f); both not amenable for angioplasty.
Interventional Management
Procedural Step
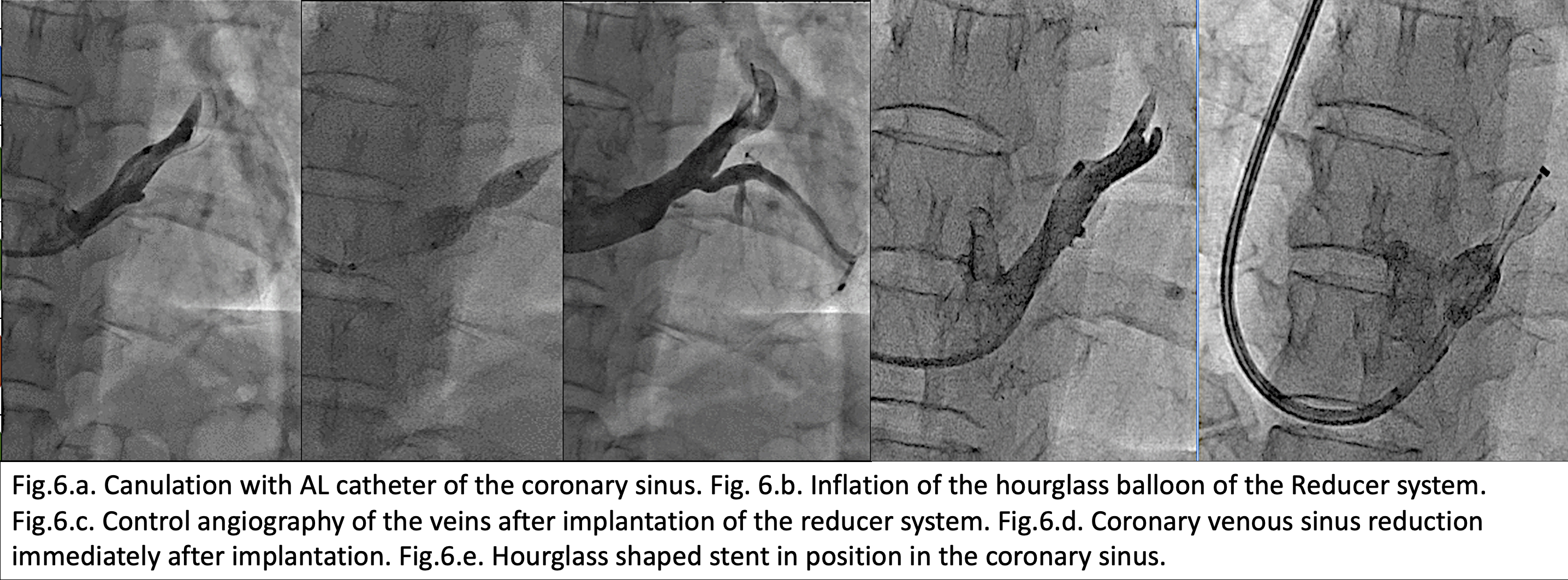
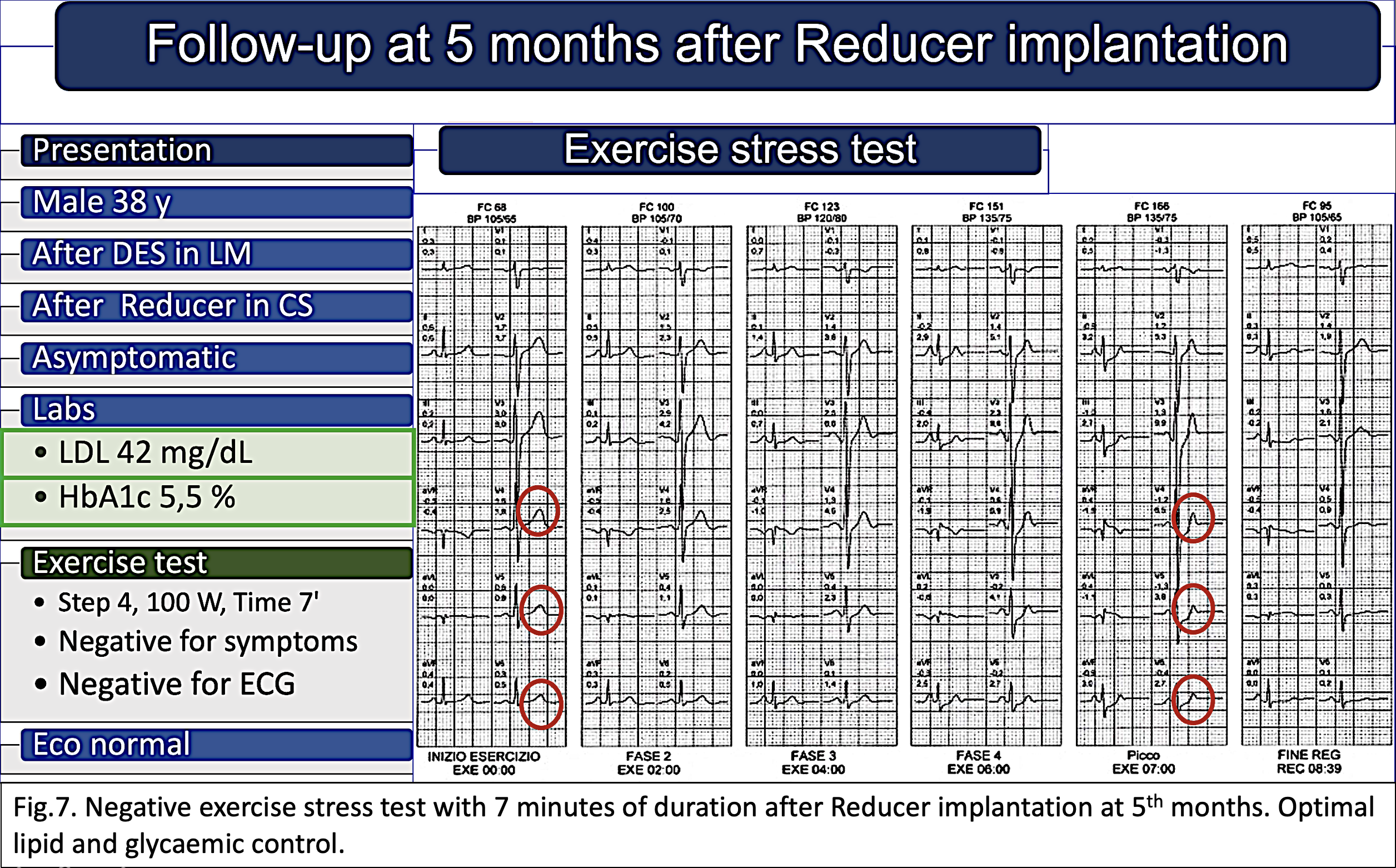
Thus, the next day after adequate hydratation to increase the venous pressure through the right jugular vein we cannulated his coronary sinus and using the child in mother technique we were able to implant successfully Neovasc coronary reducer system (Fig.6). The procedure was free of complications. The patient was discharged asymptomatic and in optimal medical therapy. At third month the patient was completely asymptomatic. His exercise stress test with duration of 7 minutes was negative for clinical end ECG criteria and also his echo stress with dobutamine was completely negative and at his clinical labs he was in optimal lipid ad glucose control (Fig. 7).
Case Summary
This case, together with our experience in the implantation of the Reducer system, confirms the clinical benefit of reducing coronary venous flow in patients with refractory angina and without options for percutaneous intervention or further modification of drug therapy.