
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-042
LAD – Diagonal Bifurcation PCI by Mini Crush Technique
By Venkata Balasubramaniyan Jayanty, Aakash Teja Durbesula
Presenter
Aakash Teja Durbesula
Authors
Venkata Balasubramaniyan Jayanty1, Aakash Teja Durbesula1
Affiliation
Sri Ramachandra Institute of Higher Education and Research, India1,
View Study Report
TCTAP C-042
CORONARY - Bifurcation/Left Main Diseases and Intervention
LAD – Diagonal Bifurcation PCI by Mini Crush Technique
Venkata Balasubramaniyan Jayanty1, Aakash Teja Durbesula1
Sri Ramachandra Institute of Higher Education and Research, India1,
Clinical Information
Patient initials or Identifier Number
Sundaravelan
Relevant Clinical History and Physical Exam
A 43 old male patient who is a diabetic for 7 years and hypertensive for 10 years came with complaints of Chest pain for 1 day duration. Chest pain is retrosternal , burning type with no radiation . It is associated with sweating . No other relevant cardiac complaints On examination, he is conscious, oriented , well built and nourished. Pulse - 64bpm , BP - 130/70 mmhg . CVS :- S1S2 heard with no murmurs. RS : Normal vesicular breath sounds heard with no added sounds.
Relevant Test Results Prior to Catheterization
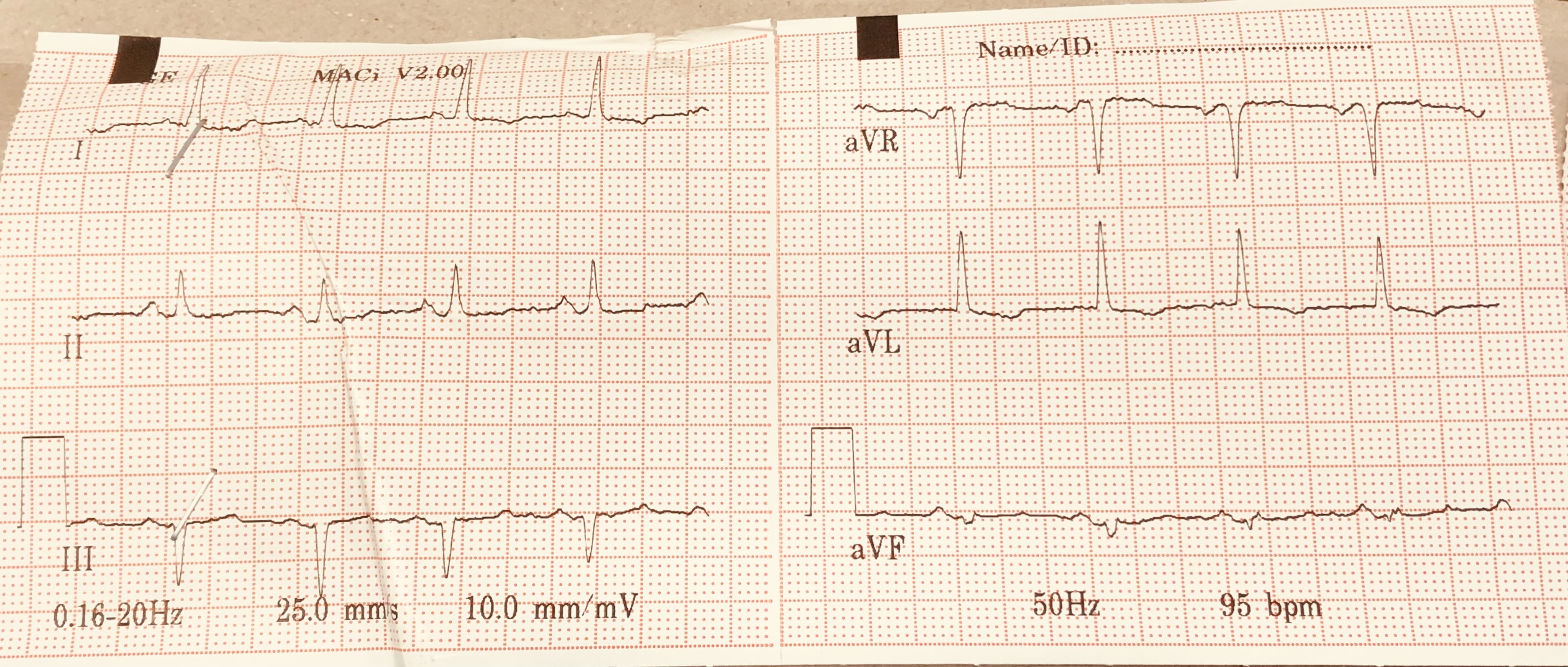
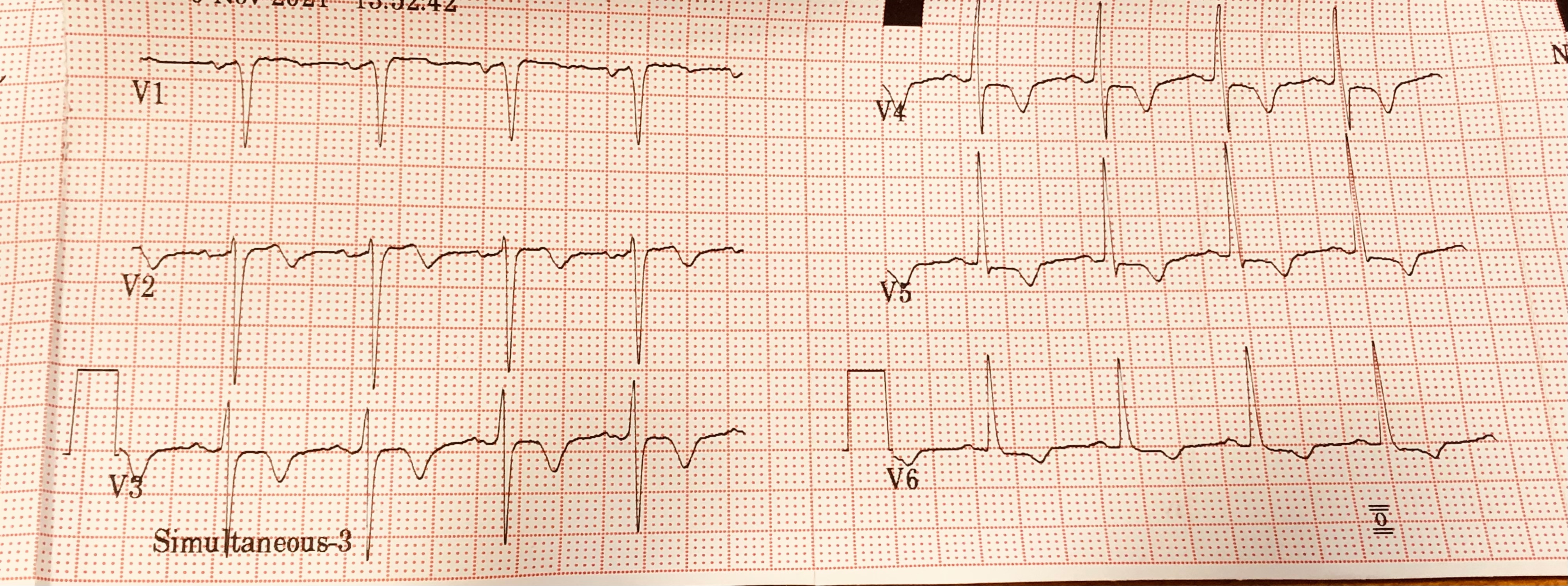
ECG: Normal sinus rythm with T wave inversions in I,AVL,V2-V6. ECHO: Normalchamber dimensions.Valvesare normal.Midanteroseptum,apical septum,lv apex,apical inferior and apical anterior wallhypokineticMildlv systolic dysfunction ( EF 45%)
Relevant Catheterization Findings
Mid LAD has thrombus-laden 90% lesion with TIMI II flow. Diagonal 1 is a medium-sized vessel with ostioproximal 90%lesion.(Medina 1,0,1). LCX - OM1 has proximal 50% lesion and it divides into superiorbranch and inferior branch.Superior branch has 50% lesion and inferior branch has 30%lesion. OM2 has proximal 30% lesion. Distal LCX has 99% subtotal occlusion.RCA-Mid RCA has long segment 50% lesion. RV branch has proximal 50-60% lesion.IMPression - CAD -Triple Vessel Disease
 se000.mpg
se000.mpg
se001.mpg
se002.mpg
Interventional Management
Procedural Step
Right radial artery wascannulated and access was secured with 7 French slender sheath. Using 7 French EBU 3.5, left coronary systemwas selectively engaged. Initially, BMW wire was used to cross the lesion and it was parked indiagonal and Runthrough wire was parked distally in LAD. Predilatation was done in LAD using 2 x 12 mmSprinter balloon at high pressure. Later, serial predilatation was done in diagonal using 1.5 x 10 mmRyurei balloon and 2 x 20 mm Sprinter balloon at nominal pressure. Later, diagonal was stented with 2.5 x 24 mmSynergy DES and LAD was stented with 2.75 x 38 mm Synergy DES successfully. Post dilatation was done in LAD with 3 x 8 mm Accuforce balloon at nominal pressure. Later, BMW wire was used to re-cross into the diagonal and due to lack of support, BMW wire was exchanged to Whisper wire for extra support. Using 1 x 10 mm Sapphire balloon was re-crossed into the diagonal and ostial flaring was done. Patient during the procedure suddenly developed transient bradycardia due to slow flow. Hence temporary pacemaker was placedin IVC as a backup . In view of thrombus in LAD, 10 ml of intracoronary Tirofiban was given. Later using 2.5 x 10 mm Sapphire NC balloon, post dilationwas done in diagonal at nominal pressure. Final kissing balloon dilatation was done using 2.5 x 10 balloon in diagonal and 2.5 x 12 mm Sapphire NC balloon in LAD simultaneously at 12 atm pressure. Check angio confirmed distal TIMI III.
se008.mpg
se016.mpg
se029.mpg
se035.mpg
se037.mpg
Case Summary
Successful bifurcation stenting using mini-crush technique was done to:
LAD using 2.75 x 38 mm synergy des and Diagonal using 2.5 x 24 mm synergy des.
Final kissing ballon dilatation was done with 2.5x 10 mm sapphire NC balloon in diagonal and 2.5 x 12 mm sapphire NC balloon in lad simultaneously at 12 atm pressure.