
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-155
Thrombosed Giant Coronary Artery Aneurysms Presenting With Ventricular Tachycardia
By Muhammad Hanis Muhmad Hamidi, Roqiah Fatmawati Abdul Kadir, Huzairi Sani, Ahmad Bakhtiar Md Radzi, Hafisyatul Aiza Zainal Abidin
Presenter
Muhammad Hanis Muhmad Hamidi
Authors
Muhammad Hanis Muhmad Hamidi1, Roqiah Fatmawati Abdul Kadir2, Huzairi Sani3, Ahmad Bakhtiar Md Radzi1, Hafisyatul Aiza Zainal Abidin1
Affiliation
Universiti Teknologi MARA (UiTM), Malaysia1, Hospital Universiti Teknologi MARA (UiTM), Malaysia2, Hospital Pantai Klang, Malaysia3,
View Study Report
TCTAP C-155
IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Non-Invasive
Thrombosed Giant Coronary Artery Aneurysms Presenting With Ventricular Tachycardia
Muhammad Hanis Muhmad Hamidi1, Roqiah Fatmawati Abdul Kadir2, Huzairi Sani3, Ahmad Bakhtiar Md Radzi1, Hafisyatul Aiza Zainal Abidin1
Universiti Teknologi MARA (UiTM), Malaysia1, Hospital Universiti Teknologi MARA (UiTM), Malaysia2, Hospital Pantai Klang, Malaysia3,
Clinical Information
Patient initials or Identifier Number
Mr MA
Relevant Clinical History and Physical Exam
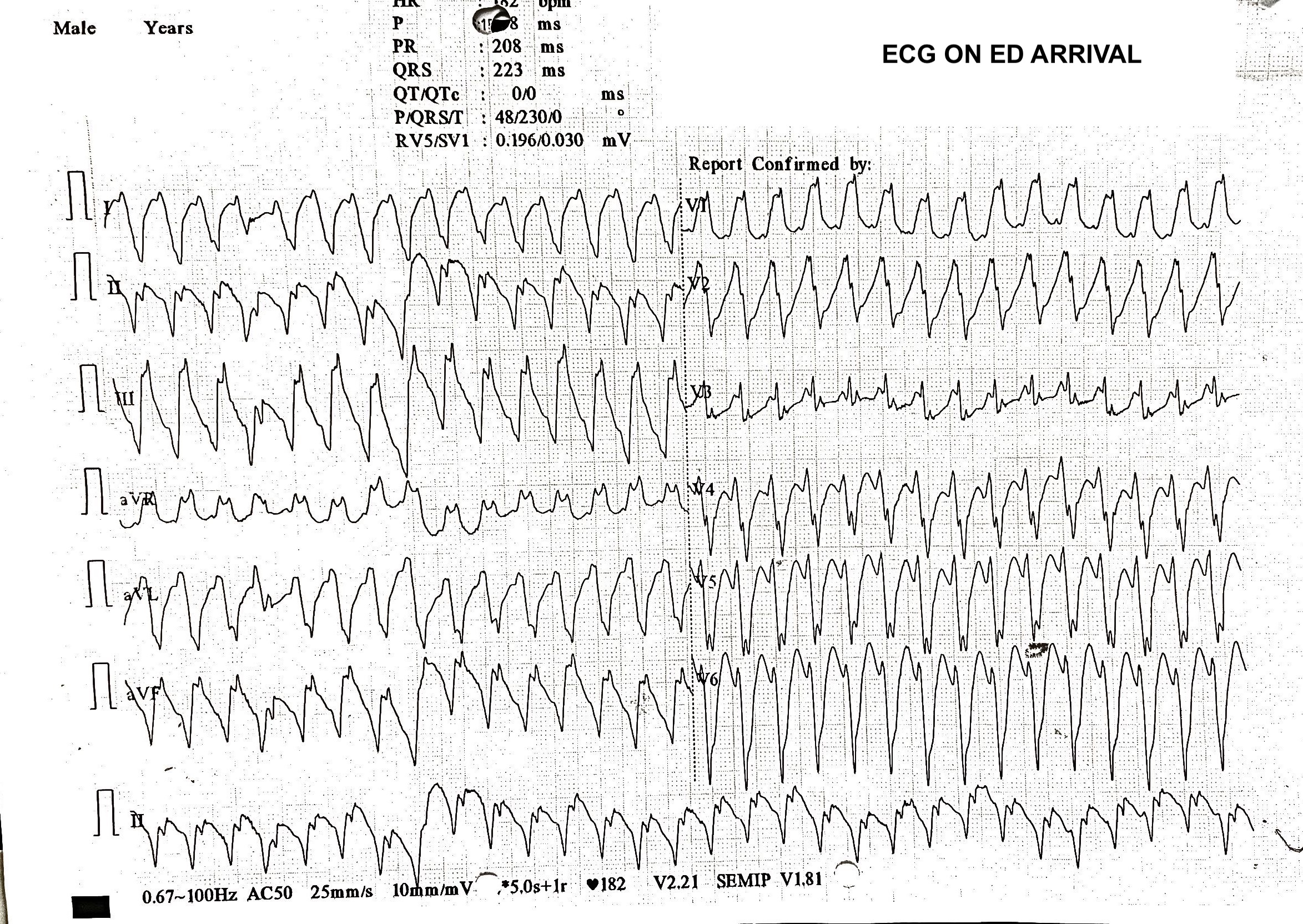
65y.o man presented with palpitation and presyncopal episode for past 3 hours. He also complained of worsening dyspnea and orthopnea for 1 month. He is a heavy smoker, has diabetes and hypertension with poor compliant to medication and follow up. In ED, vital signs were BP 108/80, HR 204, O2sats. 90%. There was bilateral lung crepitations up to mid zone. ECG showed VT. He was successfully cardioverted and intubated for respiratory distress. He was extubated after 4 days of IV diuresis in CCU.

Relevant Test Results Prior to Catheterization
In mmol/L: Urea 9.2, Creatinine 120, Na+ 134, K+ 4.2, Mg2+ 1.2, Ca2+ 2.3, Total Cholesterol 5.8, LDL-C 3.9, HDL-C 0.8, Triglyceride 2.4.HbA1c 8.8%Free T4 15.8 pmol/L. TSH 2.06 mIU/L.ECG: SR with PVC. Q waves over II,III,aVF. Poor R wave progression.Echocardiogram: LVEF 21%. Akinetic basal to apical inferolateral and inferior wall with hypokinetic the rest of LV. Presence of elliptical 46x75mm mass compressing right atrial and right basal ventricular wall with mixed echogenicity signal internally.
 ECHO PLAX RWMA.mp4
ECHO PLAX RWMA.mp4
ECHO A4C RWMA and mass.mp4
ECHO Subcostal echogenic mass.mp4
Relevant Catheterization Findings
Diagnostic catheterization showed diffuse calcified coronary artery ectatic disease with chronic total occlusion at distal LAD and proximal RCA. There is subtotal occlusion at the mid LCx with diffusely ectatic high OM1 disease.
ANGIO LAD RAO32 CRA24.mp4
ANGIO LCx CAU24.mp4
ANGIO RCA LAO44 CRA13.mp4
Interventional Management
Procedural Step
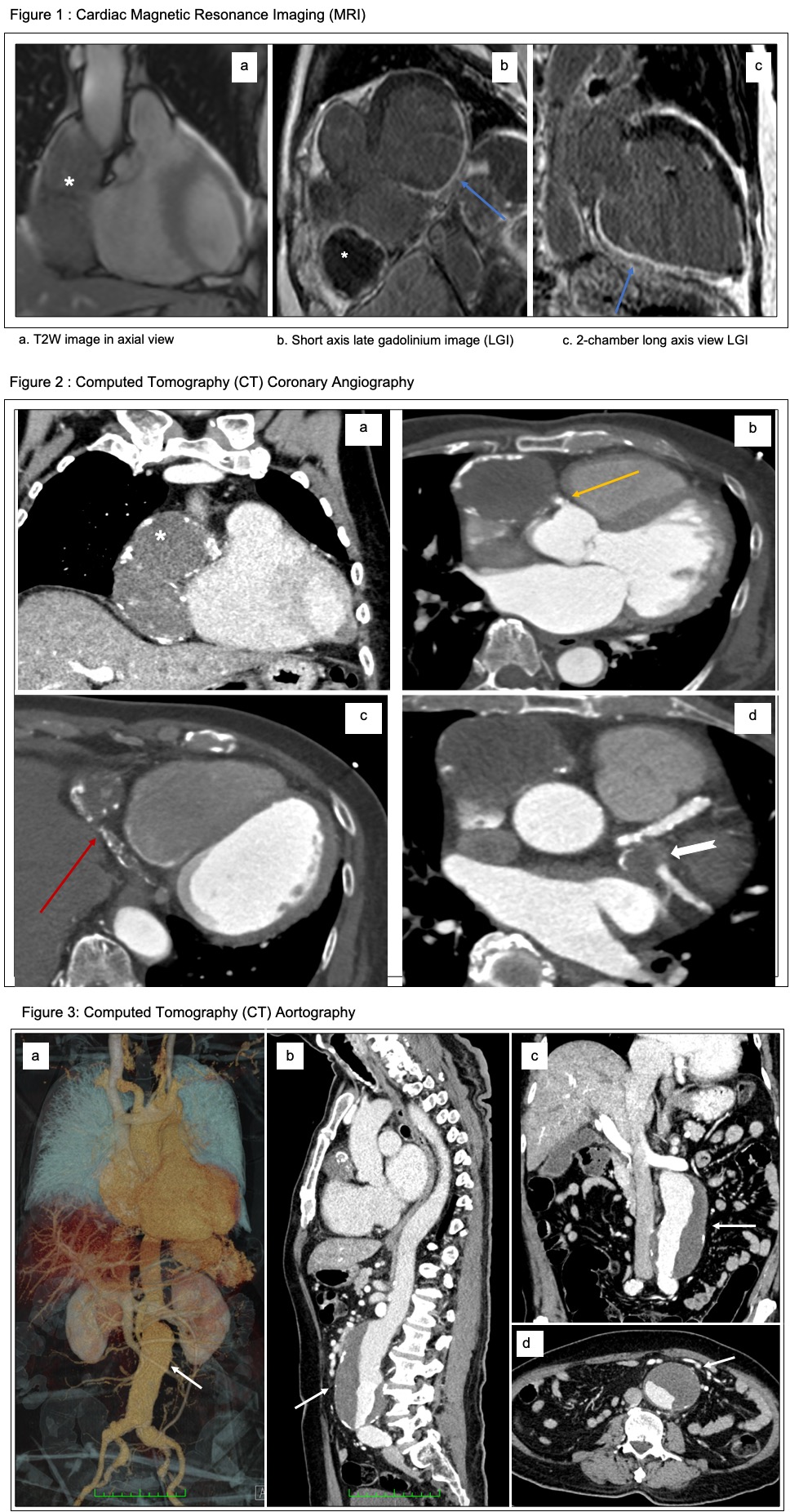
Further multimodality imaging were carried out to evaluate the pericardial mass and determine myocardial viability prior to revascularisation.
CT Coronary Angiography.mp4
Case Summary
Coronary artery aneurysms (CAA) are termed giant when the diameter exceeds the reference vessel diameter by more than 4 times. Atherosclerosis is the commonest cause of CAA in adults, whereas Kawasaki disease is responsible in pediatric population. RCA is the most affected artery (40%) followed by LAD (32%), LCx and LM being the least. This case demonstrated the usefulness of multiple imaging modalities in diagnosis and management of CAA. CT coronary angiography allows accurate evaluation of the aneurysm size and relation to other heart structures, degree of thrombus and calcification complementing the pitfall of endoluminal view from coronary catheterization alone.