
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-025
Third In-Stent Restenosis in 5 Years - Are We Doing Enough? Role of Intravascular Ultrasound and Lithotripsy in Severely Calcified ISR
By Afif Ashari, Faten Aqilah Aris, Yuen Han Lim, Azhari Rosman
Presenter
Afif Ashari
Authors
Afif Ashari1, Faten Aqilah Aris1, Yuen Han Lim1, Azhari Rosman1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-025
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Third In-Stent Restenosis in 5 Years - Are We Doing Enough? Role of Intravascular Ultrasound and Lithotripsy in Severely Calcified ISR
Afif Ashari1, Faten Aqilah Aris1, Yuen Han Lim1, Azhari Rosman1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
SS
Relevant Clinical History and Physical Exam
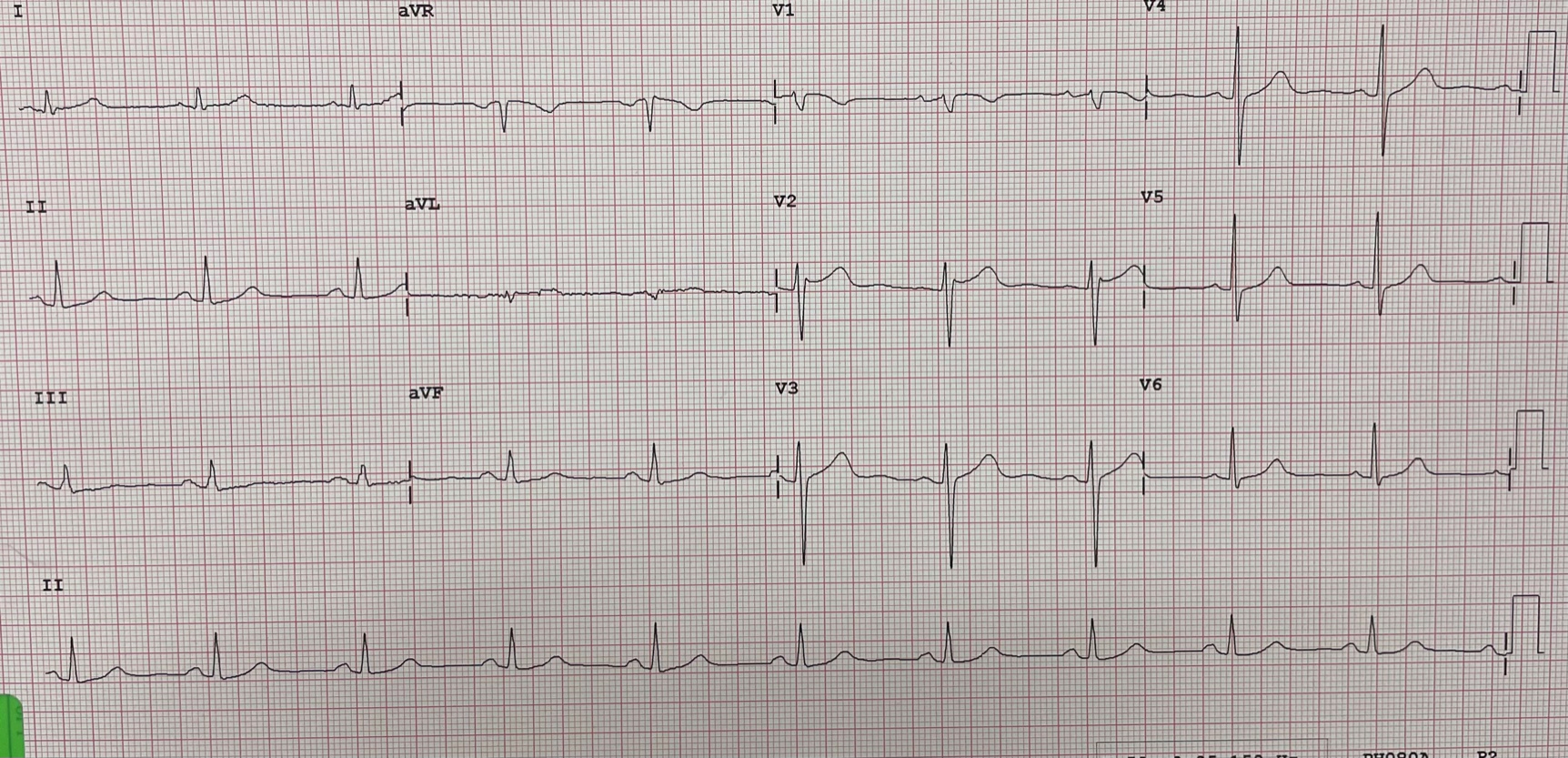
69 year old gentleman, with background history of multiple angioplasty done since 1998 (Index angioplasty done in 1998 to the LAD and RCA vessel), Diabetes mellitus, dyslipidaemia, hypertension, and chronic kidney disease IIIa.He had history of Recurrent In-stent restenosis(ISR) and angioplasty of LAD with drug coated balloon in 2016 and 2019On this occassion he was admitted with typical chest pain and treated for unstable angina.
Relevant Test Results Prior to Catheterization
Haemoglobin 13.5 g/dLCreatinine 122 micromol/LeGFR 51Trop T 109 pg/mLCreatine Kinase 196 U/LHba1c 6.7%Total cholesterol 2.9 mmol/LLDL cholesterol 1.6 mmol/L
Transthoracic echocardiogram - Borderline impaired LV impairment with LVEF 50%, anteroseptal and inferior hypokinesia. TAPSE 2.2cm. No significant valvular pathology
Transthoracic echocardiogram - Borderline impaired LV impairment with LVEF 50%, anteroseptal and inferior hypokinesia. TAPSE 2.2cm. No significant valvular pathology
Relevant Catheterization Findings
Coronary angiogram done via right radial approach
LMS - minimal distal diseaseLAD - moderate-severe diffuse ISR from ostial-proximalLCx- moderate distal diseaseRCA - minimal ISR mid segment, mild disease distal segment
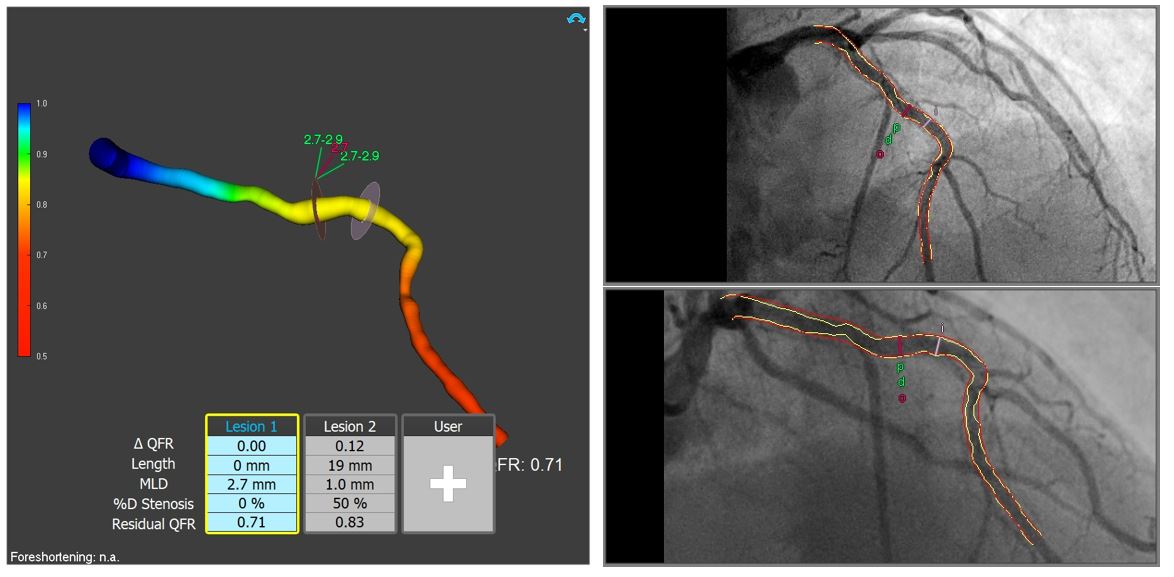
LAD vessel assessed with Quantitative Flow Reserve (QFR) - 0.71Demonstrated significant lesion therefore decided for further angioplasty for the ISR LAD
 diagnostic2.avi
diagnostic2.avi
diagnostic4.avi
LMS - minimal distal diseaseLAD - moderate-severe diffuse ISR from ostial-proximalLCx- moderate distal diseaseRCA - minimal ISR mid segment, mild disease distal segment
LAD vessel assessed with Quantitative Flow Reserve (QFR) - 0.71Demonstrated significant lesion therefore decided for further angioplasty for the ISR LAD
Interventional Management
Procedural Step
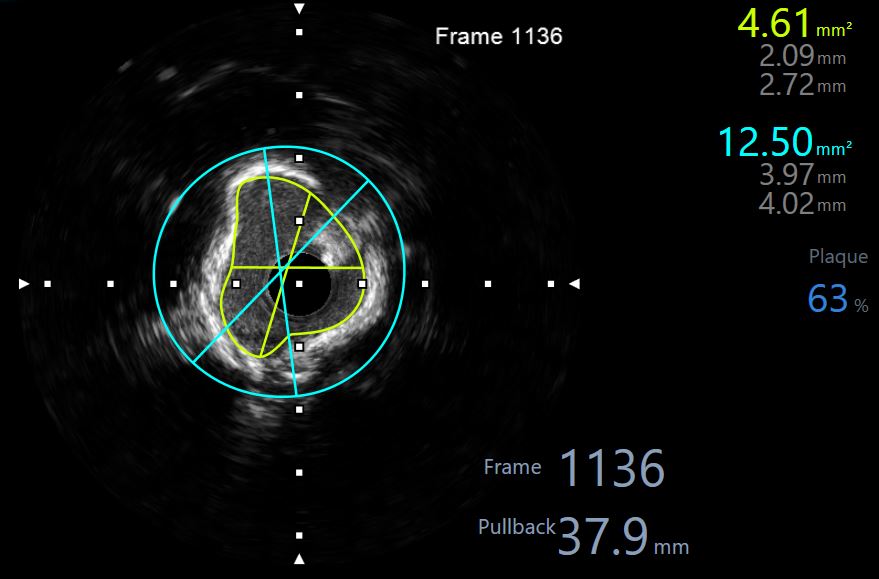
Angioplasty done to ISR LAD - IVUS guided and intravacular lithotripsy Right radial approachEBU 3.5/6Fr. Workhorse wires to LAD and diagonal branchBefore proceeding, we have investigated this lesion functionally via Quantitative flow reserve (QFR) and this demonstrated significant stenosis - with a QFR value of 0.71IVUS performed in LAD demonstrated significant circumferential calcification within the ISR with minimal luminal area of 4.61mm2. Vessel size (diameter) 3.25mm at distal edge of stent, and 4.0mm near LAD ostiumAttempted predilation with WOLVERINE 3.0/15mm cutting balloon @ 6-8atm, but unable to achieve good lesion preparationTherefore decided for IVL, with 4.0/12mm balloon @ 4atm inflation. 8x10 pulses given from ostial to mid LAD.IVUS done post predilation demonstrated multiple cracks seen within the calcified ISR lesionPredilated lesion further NC scoring balloons 3.5/15mm @ 20atm, 3.5/10mm@20atmDCB 3.5/30mm deployed @ 7atm (smaller size used to accommodate heavy plaque burden)Good angiographic results with TIMI III flow. And final IVUS done showed MLA proximal has improved to 7mm2
pci - final 3.avi
pci - final 1.avi
Case Summary
Especially in recurrent ISR cases, it is important to investigate 'stent failure' with intravascular ultrasound. This case demonstrated severe heavy calcification that was likely inadequately prepared before previous drug coated balloon angioplasties.
In calcified ISR lesions, we need to consider IVL as a modality to modify the lesion better especially if we consider atherectomy is technically contraindicated within ISR lesions
The utility of Quantitative Flow Reserve (QFR) to assess borderline lesions. This case demonstrated diffuse moderate-severe ISR from ostial to proximal LAD, but the QFR confirmed the lesion is significant and requires further intervention.