
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-111
Successful “Ping-pong” Technique by Placing a Polytetrafluoroethylene-Covered Stent Followed by Inflation of Ryusei, a Perfusion Balloon for Type-3 Perforation at Proximal Right Coronary Artery Complicated Immediately After High-Pressure Dilations Inside Xience Skypoints
By Keisuke Kajitani, Tetsuya Ishikawa, Kahoko Mori, Hidehiko Nakamura, Hideyuki Aoki, Yukiko Mizutani, Tatsuhiko Ito, Yuta Kimura, Yuta Kikuchi, Tomoaki Ukaji, Kota Yamada, Itaru Hisauchi, Shiro Nakahara, Yuji Itabashi, Sayuki Kobayashi, Isao Taguchi
Presenter
Hironori Kajitani
Authors
Keisuke Kajitani1, Tetsuya Ishikawa2, Kahoko Mori1, Hidehiko Nakamura1, Hideyuki Aoki1, Yukiko Mizutani1, Tatsuhiko Ito1, Yuta Kimura1, Yuta Kikuchi1, Tomoaki Ukaji1, Kota Yamada1, Itaru Hisauchi1, Shiro Nakahara1, Yuji Itabashi1, Sayuki Kobayashi1, Isao Taguchi1
Affiliation
Dokkyo Medical University, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2,
View Study Report
TCTAP C-111
CORONARY - Complications
Successful “Ping-pong” Technique by Placing a Polytetrafluoroethylene-Covered Stent Followed by Inflation of Ryusei, a Perfusion Balloon for Type-3 Perforation at Proximal Right Coronary Artery Complicated Immediately After High-Pressure Dilations Inside Xience Skypoints
Keisuke Kajitani1, Tetsuya Ishikawa2, Kahoko Mori1, Hidehiko Nakamura1, Hideyuki Aoki1, Yukiko Mizutani1, Tatsuhiko Ito1, Yuta Kimura1, Yuta Kikuchi1, Tomoaki Ukaji1, Kota Yamada1, Itaru Hisauchi1, Shiro Nakahara1, Yuji Itabashi1, Sayuki Kobayashi1, Isao Taguchi1
Dokkyo Medical University, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2,
Clinical Information
Patient initials or Identifier Number
K S
Relevant Clinical History and Physical Exam
A 83-year-old male wasintroduced to our institute owing to the severely calcified coronary arteriesby general plane computed tomography (CT) and the history of cerebralinfarction with the stenosis of cervical artery. His diabetes history was morethan 20 years (HbA1c 7.4%), and other coronary risk factors were hyperlipidemia(TC 244 mg/dl, TG 189 mg/dl, HDL-C 57 mg/dl, and LDL 164 mg/dl), hypertension,and past smoking (Hb16.3 g/dl, Cre 0.87 mg/dl).

Relevant Test Results Prior to Catheterization
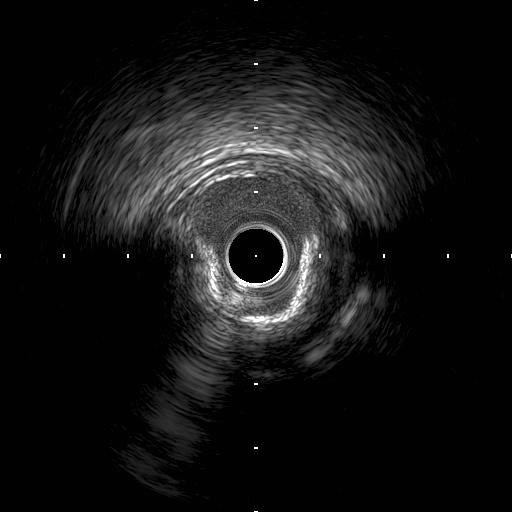
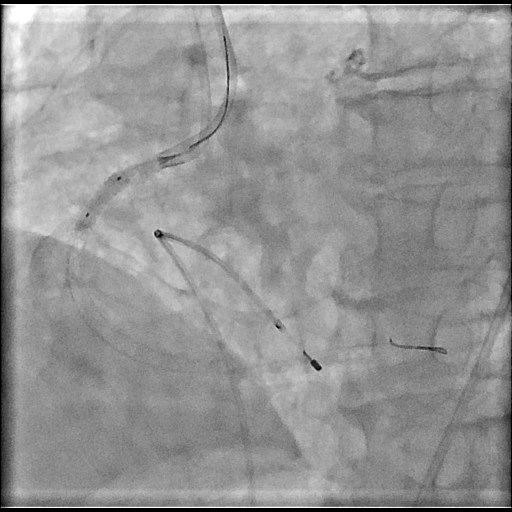
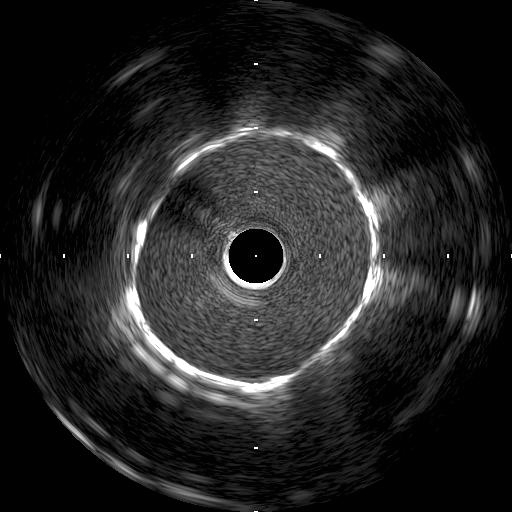
InRCA (Figure 1), there was a diffuse stenosis from ostium to theproximal-portion (Lesion-1), and spot 90% stenosis in mid-portion (Lesion-2). Elective PCI was undergone by inserting a7Fr glidesheath via right radial artery, a guiding catheter (7Fr Champ1.5SH). Intravascular images showed the severelycalcification (Figure 2 for Lesion 1). Orbital atherectomy wasapplied along the diffuse calcifiedplaques. However, calcified plaques at proximal site was not fully modified(Figure 3)

Relevant Catheterization Findings
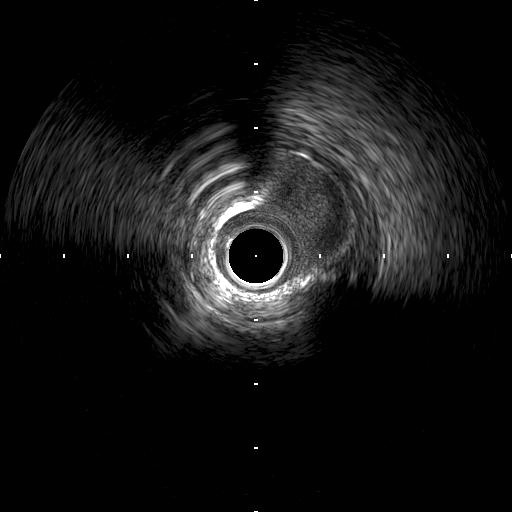
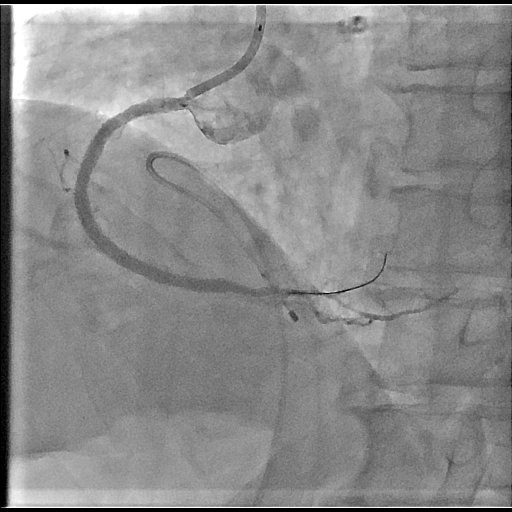
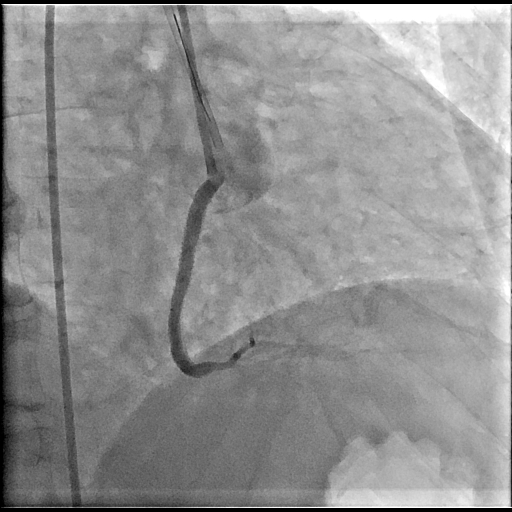
Rotational atherectomy (burrsize 1.75mm) was undergone. Rotablator made superficial irregular lumensmooth (Figure 4). After 3-mm sized balloon dilations, XienceSkypoint (4x48 and 4x38 mm) were placedincluding ostium (Figure 5). Post-dilations using anon-compliant balloon (Raiden 4.5x15mm) were undergone. Immediately, coronaryperforations with multiple blowout flows classified as Ellis-classification type-3were occurred (Figure 6). Perforated lesion was suppressed by Raiden.


Interventional Management
Procedural Step
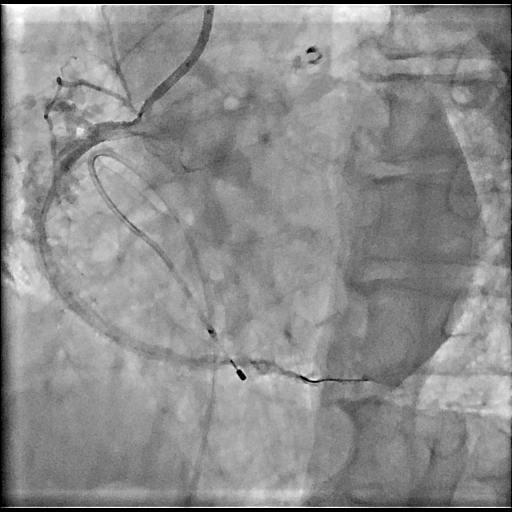
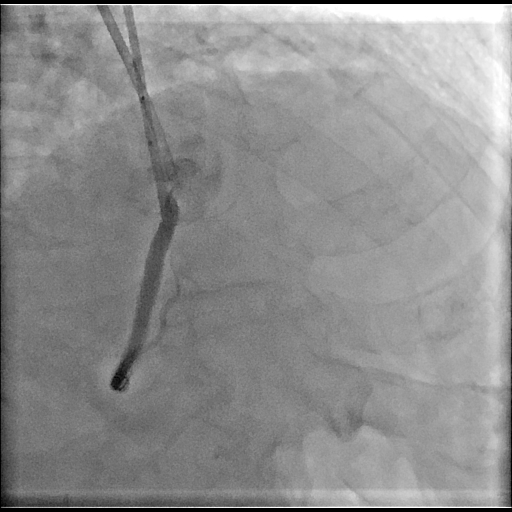
Raiden was exchanged to Ryusei,a perfusion balloon, inside Xience stent, suppressing the blowouts.Concurrently, a guiding catheter JR4 was nearly engaged to RCA via rightfemoral artery (Figure 7). Since activated clotting time was 154s, protaminewas not administered. Temporarily, Ryusei was deflating, and a GW (Sion blue)from the new system was crossed. Before removing Ryusei, oozing sites wereascertained, a polytetrafluoroethylene-covered stent (GraftMaster2.8x16mm) was prepared and rapidly deployed (Figure 8). After post-balloondilations by using NC Emerge (5x15mm) with 12 atmospheres (Figure 9),perforations were once ceased. IVUS images showed that GraftMaster tightlydilated inside Xience. However, along the perforated lesion, reference vessel diameterwas observed to be more than 8mm (Figure 10). The echocardiography did not showthe apparent pericardial effusion. A few minutes later, oozing flow recurred(Figure 11). Thus, GraftMaster was further dilated by using a 5.5mm-sized NCEmerge. The interval for these bailout proceduresfrom perforation to ascertain the cessation was 32 minutes. Finally, TIMI grade flow of 3 with good Xience dilationwas obtained in RCA (Figures 12). After the procedure, the maximum serum valueof CK was 750 (IU/dl) without accumulating pericardial effusion. He dischargedat the post-PCI days of 4.
Case Summary
We successful bailed out from the Ellisclassification type-3 acute perforations by alternatively inflating Ryusei, aperfusion balloon, prior to sealing a polytetrafluoroethylene-covered stent (“Ping-pong”technique) occurred immediately after rated pressure of 22 atmosphere dilationsusing a 4.5mm-sized non-compliant balloon inside Xience Skypoint Stent placedfor diffuse severely calcified proximal right coronary artery followed byorbital and rotational atherectomies.