
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-126
Optical Coherence Tomography Guided Covered Stent Treatment of Coronary Artery Aneurysm
By Gavin Ng, Hui Wen Sim, Adrian Low
Presenter
Gavin Ng
Authors
Gavin Ng1, Hui Wen Sim1, Adrian Low1
Affiliation
National University Heart Centre, Singapore1,
View Study Report
TCTAP C-126
CORONARY - Stents (Bare-metal, Drug-eluting)
Optical Coherence Tomography Guided Covered Stent Treatment of Coronary Artery Aneurysm
Gavin Ng1, Hui Wen Sim1, Adrian Low1
National University Heart Centre, Singapore1,
Clinical Information
Patient initials or Identifier Number
Mr. MR
Relevant Clinical History and Physical Exam
A 66 year-old male with a background of hypertension, hyperlipidemia and smoking has a history of ischemic heart disease. He previously had an acute myocardial infarction in 2013 for which he underwent drug eluting stent placement in his left anterior descending artery (LAD) and left circumflex artery (LCx) respectively. There was a large coronary artery aneurysm in the LAD and he was started on warfarin. He presented in 2019 with a Non-ST elevation myocardial infarction.
 Pre PCI LAD 2013.mp4
Pre PCI LAD 2013.mp4
Post PCI LAD 2013.mp4
Relevant Test Results Prior to Catheterization
An echocardiogram showed a left ventricular ejection fraction of 50% with regional wall motion abnormality seen in the inferior walls. Laboratory investigations showed mildly impaired renal function and a normal full blood count. Warfarin was stopped and patient was started on aspirin and plavix in preparation for the coronary angiogram.
Relevant Catheterization Findings
The coronary angiogram performed showed patent stents in the LAD and LCx. There was a de novo high grade lesion in the distal right coronary artery (RCA) and the LAD coronary artery aneurysm had increased in size from 1.4 cm to 2.2 cm. A heart team discussion was done and decision was made to perform percutaneous coronary intervention (PCI) to the RCA and for covered stent closure of the giant saccular coronary aneurysm in the LAD. The patient had declined any surgical discussion.
Pre PCI RCA 2019.mp4
Post PCI RCA 2019.mp4
Pre PCI LAD.mp4
Interventional Management
Procedural Step
Initial vascular access was obtained by inserting a 6 Fr slender sheath into the left radial artery. The right coronary ostium was cannulated with a 6 Fr JR 4 guide catheter. A Sion Blue guidewire was used to cross the lesion which was subsequently predilated with a 2.5 x 15 mm Ikazuchi balloon. This facilitated the passage of the Dragonfly Optis catheter and the fibrocalcific lesion was prepared with a 4.0 x 13 mm Lacrosse balloon. The lesion was then stented with a 5.0 x 24 mm drug eluting stent with optical coherence tomography (OCT) guidance. Post dilation was done with a 5.5 x 15 mm NC Emerge balloon.
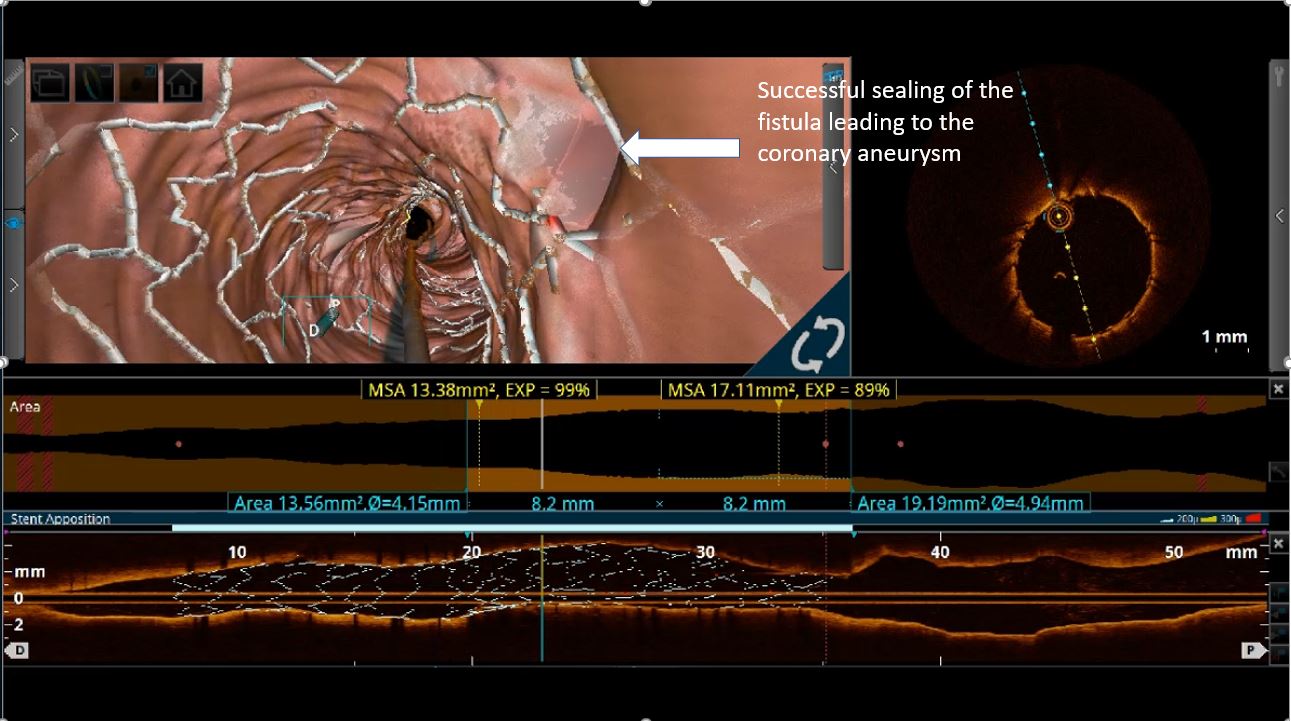
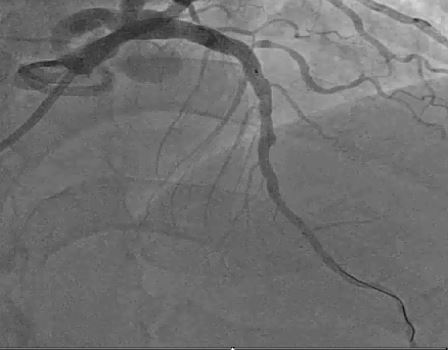
The left coronary ostium was cannulated with a 6 Fr EBU 4.0 guide catheter. The Sion Blue guidewire was used to advance into the distal LAD. OCT was performed to clarify the fistula opening, size and position. This demonstrated a single feeding fistula into the aneurysm with a 2.8 mm opening just proximal to the previous stent. Utilizing a Crusade double lumen microcatheter, a Runthrough Hypercoat guidewire was used to cross into the aneurysm to facilitate accurate placement of the covered stent. A 4.5 x 15 mm PK Papyrus covered stent was deployed across the mouth of the fistula and this was post dilated with a 5.0 x 6 mm Accuforce balloon to 18 atmospheres. Final OCT run demonstrated satisfactory stent expansion and apposition and sealing of the feeding fistula to the LAD coronary aneurysm. Angiogram demonstrated brisk TIMI III flow in the LAD once the aneurysm was sealed.

The left coronary ostium was cannulated with a 6 Fr EBU 4.0 guide catheter. The Sion Blue guidewire was used to advance into the distal LAD. OCT was performed to clarify the fistula opening, size and position. This demonstrated a single feeding fistula into the aneurysm with a 2.8 mm opening just proximal to the previous stent. Utilizing a Crusade double lumen microcatheter, a Runthrough Hypercoat guidewire was used to cross into the aneurysm to facilitate accurate placement of the covered stent. A 4.5 x 15 mm PK Papyrus covered stent was deployed across the mouth of the fistula and this was post dilated with a 5.0 x 6 mm Accuforce balloon to 18 atmospheres. Final OCT run demonstrated satisfactory stent expansion and apposition and sealing of the feeding fistula to the LAD coronary aneurysm. Angiogram demonstrated brisk TIMI III flow in the LAD once the aneurysm was sealed.
Case Summary
This case report showcases the effective treatment of a giant saccular coronary artery aneurysm by a covered stent. OCT can guide the precise deployment of the appropriately sized stent and optimize the PCI result by ensuring that the stent is well apposed and expanded. At 18 month review, the patient remains well with no reported symptoms. He had other coronary artery to pulmonary artery fistulas which were treated conservatively. Covered stent treatment is a viable alternative for patients with coronary aneurysms who declined surgery.