
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-084
Percutaneous Coronary Intervention in an Occluded Saphenous Vein Graft
By Adelyn Nisha Henry, Hou Tee Lu, Kumutha Gobal, Vicknesan Kulasingham, Heng Shee Kim, Choon Keong Tee
Presenter
Adelyn Nisha Henry
Authors
Adelyn Nisha Henry1, Hou Tee Lu1, Kumutha Gobal1, Vicknesan Kulasingham2, Heng Shee Kim1, Choon Keong Tee1
Affiliation
Sultanah Aminah Hospital, Malaysia1, Ministry of Health Malaysia, Malaysia2,
View Study Report
TCTAP C-084
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Percutaneous Coronary Intervention in an Occluded Saphenous Vein Graft
Adelyn Nisha Henry1, Hou Tee Lu1, Kumutha Gobal1, Vicknesan Kulasingham2, Heng Shee Kim1, Choon Keong Tee1
Sultanah Aminah Hospital, Malaysia1, Ministry of Health Malaysia, Malaysia2,
Clinical Information
Patient initials or Identifier Number
Patient A
Relevant Clinical History and Physical Exam
A 70-year-old gentleman presented to our Emergency department with daily chest pain at rest and exertionThis had intensified over the last 3 weeks. He has a background history of Hypertension, Atrial Fibrillation, Chronic Kidney Disease and smoking. In 2016, patient underwent a CABG with 2 grafts, SVG- posterior descending artery and a SVG- Left anterior descending artery. He also had a mechanical mitral valve replacement in 2016 with a 25MM St. Jude mechanical valve.He was in NYHA class 2.
Relevant Test Results Prior to Catheterization
Electrocardiogram showed rate controlled atrial fibrillation with a heart rate of 60 beats/minute.Transthoracic echocardiogram demonstrated an EF: 59%, dilated LV/LA with a Mild AR/TR. The mechanical mitral valve was intact with no leak seen. Renal function was impaired with a creatinine clearance of 45mls/min/1.73m2Cardiac enzymes were not elevated.A diagnosis of unstable angina was made.
Relevant Catheterization Findings
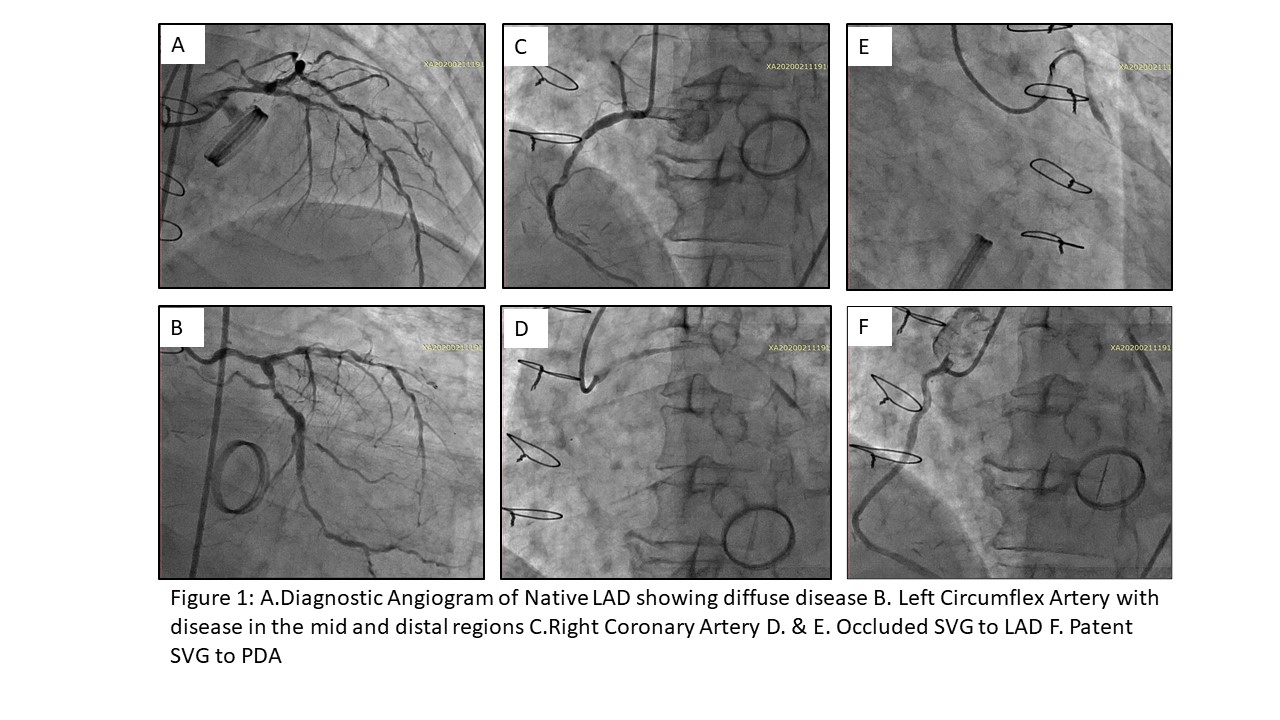
His coronary angiogram revealed diffuse disease of his native Left Anterior Descending artery. His Left Circumflex artery had moderate stenosis in the mid and distal regions of around 70-80%.His Right Coronary artery had around 60% disease in the mid region. His SVG graft-PDA was patent however his SVG-LAD was diffusely degenerated across the entire length with slow flow from the proximal segment(FIG. 1D&E)
Interventional Management
Procedural Step
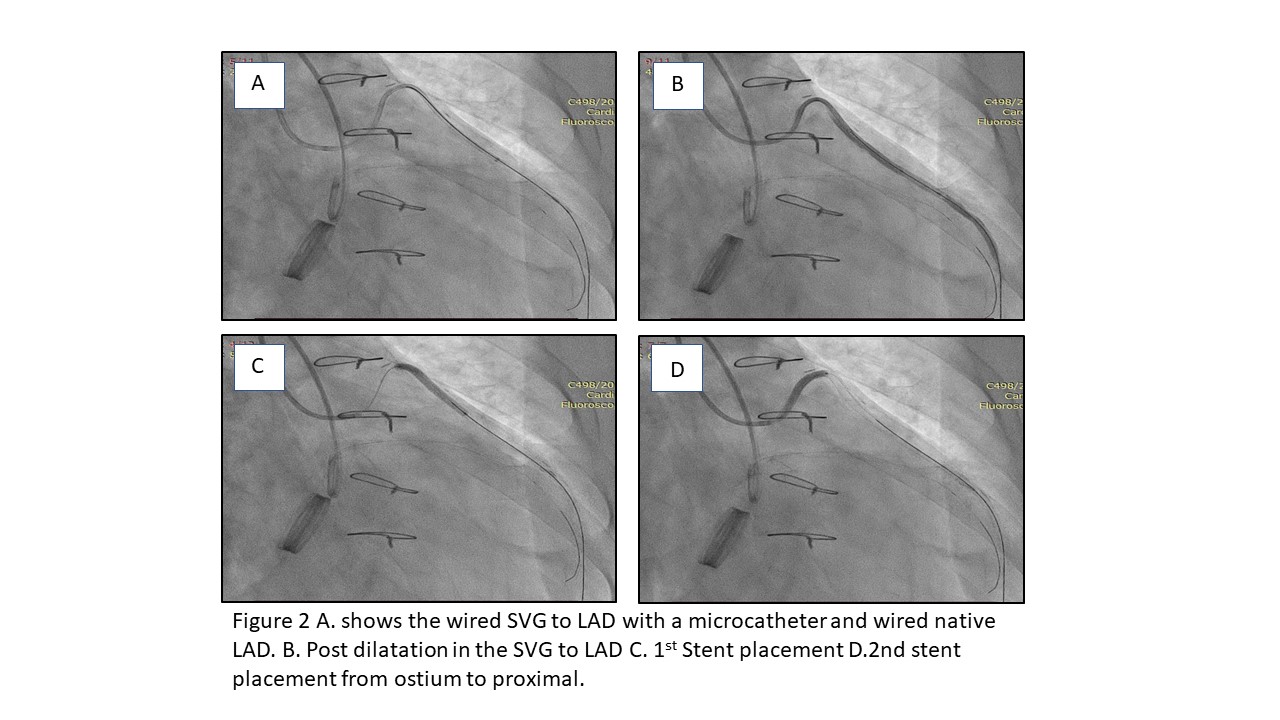
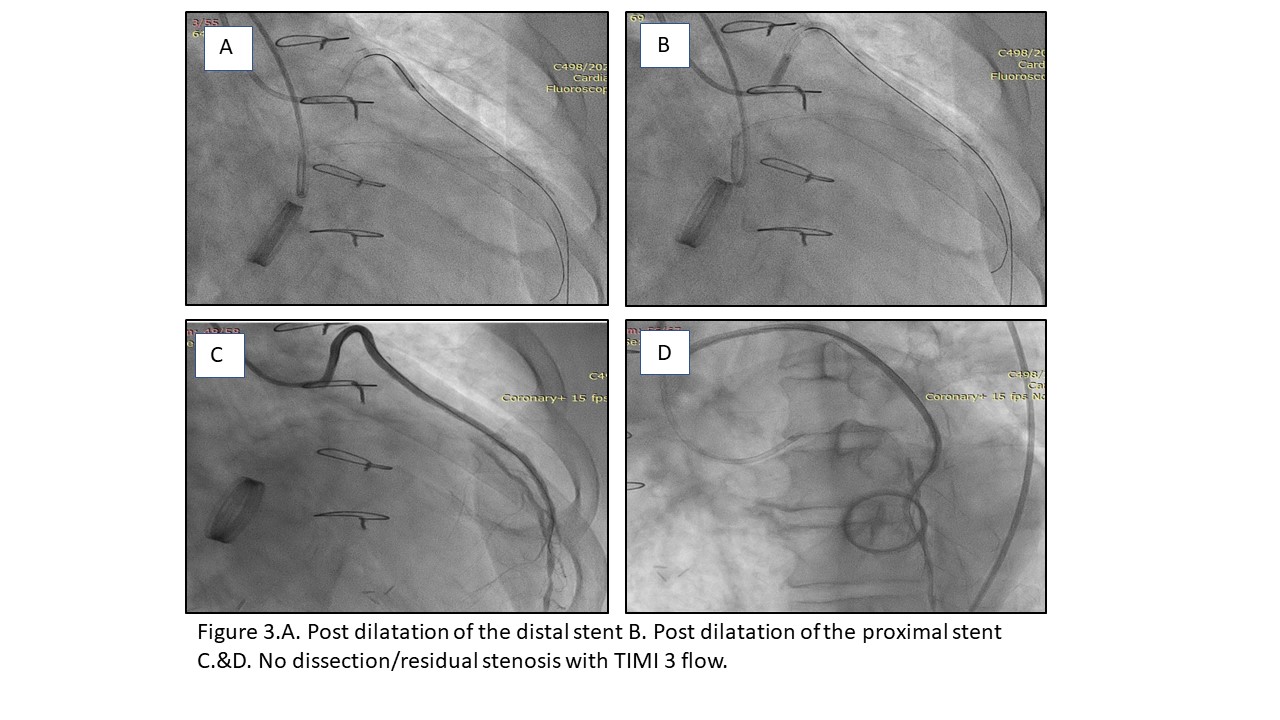
Patient was given 7000 units of heparin(100units/kg), the SVG graft was cannulated via Right femoral approach with a JR4-6F guide catheter(Medtronic, USA). The native left system was engaged with an EBU 3.0-6F(Medtronic, USA) via the Right radial artery and wired using a BMW Universal™ Guidewire(Abbot Vascular).The SVG graft was wired using a Runthrough® Intermediate (Terumo Corporation), supported with MOGUL (microcatheter, NIPRO). There was difficulty crossing, the wire was escalated to Fielder® XT-A(Asahi Intecc, Japan) and the wire tip was placed in the distal SVG graft.Due to poor support, there was difficulty delivering the pre dilatation balloon.A GUDIEZILLA™ Guide Extension Catheter(Boston Scientific, USA) was used to reach the anastomotic site.Predilated from distal to proximal using IKAZUCHI Zero™ 1.0X6 (KANEKA, Japan) Followed by a NC EUPHORA™ 2.0x10(Medtronic, USA) at 14atm for 20 seconds. Stented using XIENCE Xpedition™ 2.5x48 (Abbot Vascular) deployed at 14atm(FIG. 2C) Post dilated with Pantera LEO 3.0X15 (BIOTRONIK, Germany) at 12atm for 20 seconds.A type 3 dissection was seen proximal to the stent edge, it was not flow limiting. Predilated from the proximal SVG graft to the ostium using a Pantera LEO 3.0x 15( BIOTRONIK, Germany) at 14 atm Stented using XIENCE Xpedition™ 3.0X48(Abbot Vascular) deployed at 11 atm(FIG. 2D)Post procedure angiogram had TIMI 3 flow in the SVG-LAD graft and the anterograde limb of the LAD filled up to its mid segment(FIG.3D &E)
Case Summary
Due to the increasing number of coronary bypass grafting being performed, we see an ever increasing number of vein graft occlusions.The site of anastomosis of a vein graft to the native vessel predisposes to occlusion.In many patients a re-do CABG is not an optionIn symptomatic patients an attempt to PCI to a SVG intervention may remain a complex but feasible only option.