
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-002
A Case of Very Late Stent Thrombosis
By Yik Ching Hung
Presenter
Yik Ching Hung
Authors
Yik Ching Hung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1,
View Study Report
TCTAP C-002
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
A Case of Very Late Stent Thrombosis
Yik Ching Hung1
Tuen Mun Hospital, Hong Kong, China1,
Clinical Information
Patient initials or Identifier Number
CFS
Relevant Clinical History and Physical Exam
74-year-old male with received PCI for angina in 2015. Angiogram showedmid LAD CTO, LCx and OM3 bifurcation lesion and mid RCA 95% disease. Stentswere placed in RCA and LCx to OM. Two overlapping stents were placed in LADafter antegrade wiring (Orsiro 2.5/30, Orsiro 2.25/40).
Admitted 8/11/2021 for chest pain, onset 4 days ago.
Ongoing chest pain, brought to lab on 11/11/2021.
Admitted 8/11/2021 for chest pain, onset 4 days ago.
Ongoing chest pain, brought to lab on 11/11/2021.
Relevant Test Results Prior to Catheterization
He was started on dual antiplatelet and subtaneouslow molecular weight heparin.
ECG showed q wave at anterior leads, Trop I greater than 50000 ng/L. Echoshowed impaired LV systolic function (LVEF 38%), hypokinetic mid to basalanterior and septal wall, as well as akinetic apex.
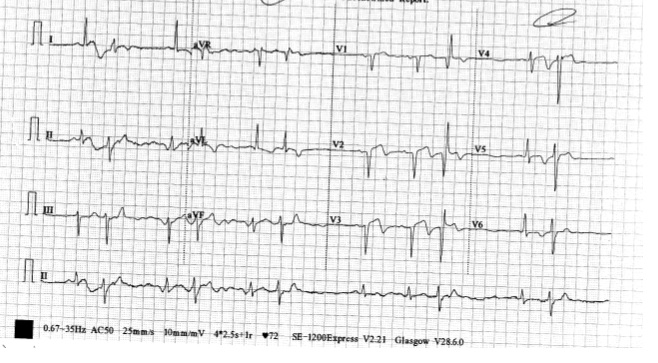
ECG showed q wave at anterior leads, Trop I greater than 50000 ng/L. Echoshowed impaired LV systolic function (LVEF 38%), hypokinetic mid to basalanterior and septal wall, as well as akinetic apex.
Relevant Catheterization Findings
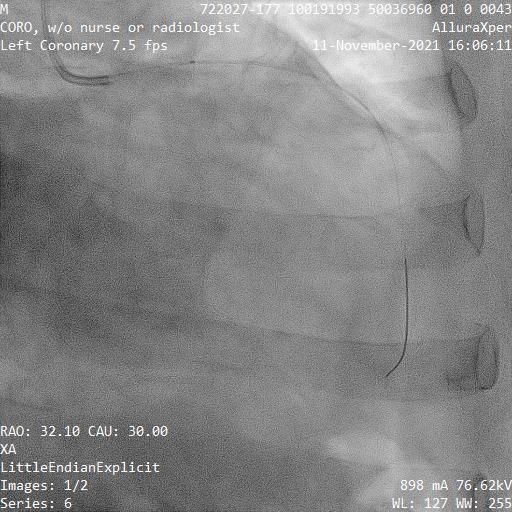
Angiogram showed filling defect over LAD proximalstent edge, rest of the stent being patent. LCx to OM stent patent, withaneurysm at distal LCx just before bifurcation followed by subtotal occlusion.RCA stent also patent, with retrograde filling to LCx.
 mov-series-003-Left Coronary 7.5 fps.wmv
mov-series-003-Left Coronary 7.5 fps.wmv
Interventional Management
Procedural Step
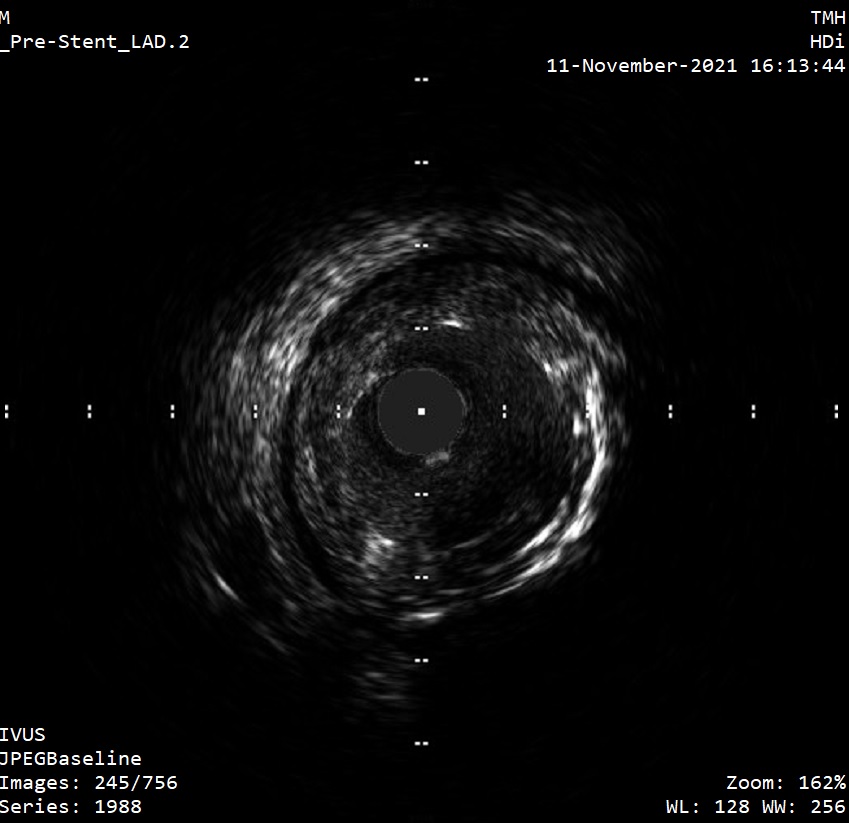
Left system engaged with EBU3.5, LAD wired withRunthrough NS. Clot aspiration done by Export Advance catheter for 4times. Angiogram showed reduced clot burden. IVUS showed mild residue clotover proximal stent edge, no in-stent restenosis seen. It also revealedunderexpansion of old stent, with a vessel size of around 3.25 mm.
Proximal stent edge further dilated with Raiden 2.75/10 and Accuforce 3.0/8 NCballoon. Good stent expansion confirmed by IVUS and distal flow was good.Proximal to mid LAD stented with Orsiro 3.0/18. IVUS guided post-stentingoptimization done. Remained TIMI III flow.
mov-series-007-Left Coronary 7.5 fps.wmv
Proximal stent edge further dilated with Raiden 2.75/10 and Accuforce 3.0/8 NCballoon. Good stent expansion confirmed by IVUS and distal flow was good.Proximal to mid LAD stented with Orsiro 3.0/18. IVUS guided post-stentingoptimization done. Remained TIMI III flow.
Case Summary
We report a case of STEMI caused by very late stentthrombosis. The cause of thrombosis is underexpansion of stent following achronic total occlusion PCI. This suggests restudy of coronary angiogram may benecessary following chronic total occlusion PCI as positive remodeling ofvessels can occur later.