
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-026
Unexpected Accordion: To Burr, or not to Burr
By Cliff Li, Hee Hwa Ho
Presenter
Ki Fung Cliff Li
Authors
Cliff Li1, Hee Hwa Ho1
Affiliation
Tan Tock Seng Hospital, Singapore1,
View Study Report
TCTAP C-026
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Unexpected Accordion: To Burr, or not to Burr
Cliff Li1, Hee Hwa Ho1
Tan Tock Seng Hospital, Singapore1,
Clinical Information
Patient initials or Identifier Number
D.L.
Relevant Clinical History and Physical Exam
Mr D.L is a 52 year old male with a past medical history of smoking and piles. He presented with 2 week history of intermittent chest pain which worsened over last 2 days. On examination in emergency department, BP 115/67 PR 87 SpO2 98% on room air. Clinical examination was uneventful with dual heart sounds and clear lung sounds.
Relevant Test Results Prior to Catheterization
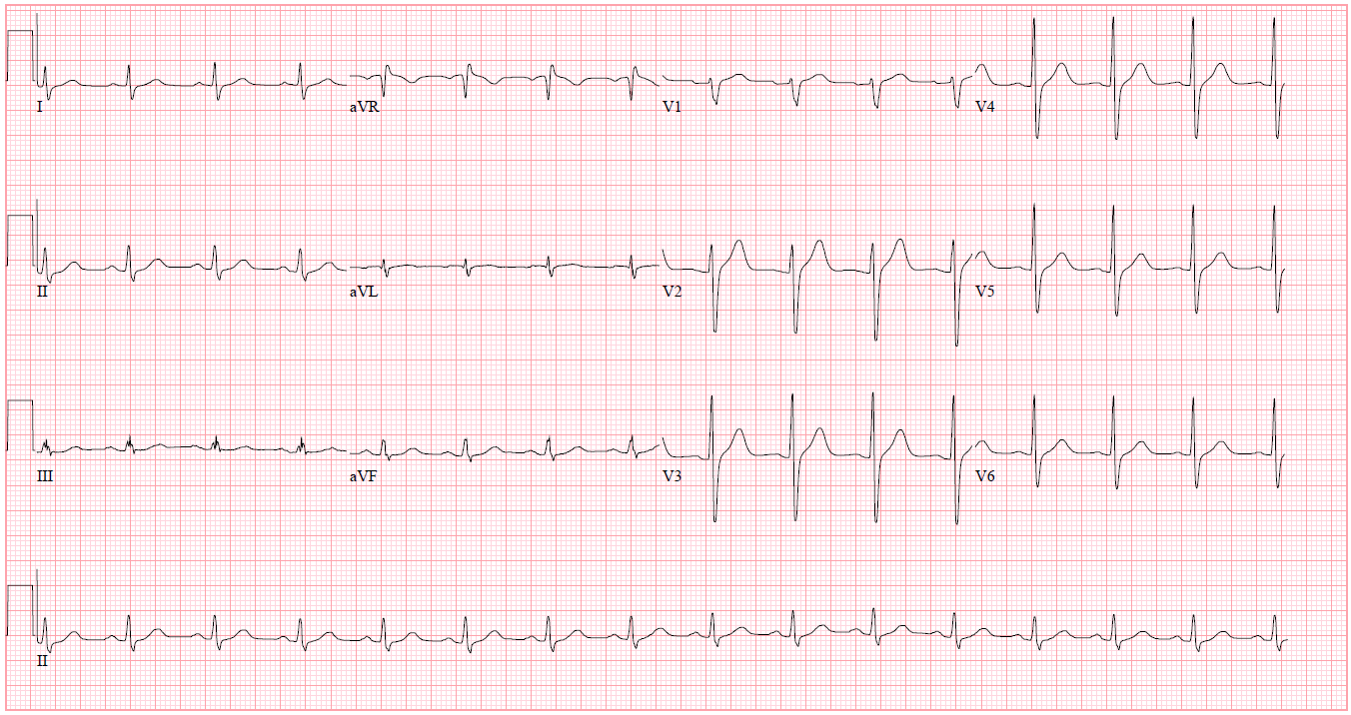
Electrocardiogram shows sinus rhythm with no significant ST segment abnormalities. High sensitivity Troponin I was raised with increasing trend from 479 to 540 ng/L.
Relevant Catheterization Findings
Coronary angiogram shows significant triple vessel disease with heavily calcification in LAD and RCA. Heavily calcified mid LAD 85% stenosis, mid LCx 90% stenosis with calcified and tortuous mid RCA 80% stenosis.
 211101 - Accordion IVL - LAD 1.Ser1.avi
211101 - Accordion IVL - LAD 1.Ser1.avi
211101 - Accordion IVL - Cx.Ser1.avi
211101 - Accordion IVL - RCA.Ser1.avi
Interventional Management
Procedural Step
Patient declined CABG and hence multivessel PCI proceeded. LAD was treated with orbital atherectomy and drug-coated balloon (DCB) with reduction of stenosis to <30%. LCx was also treated with DCB and residual stenosis 30%. Staged PCI to RCA was done 3 days later. Due to severe calcification and tortuosity, we preferred rotational atherectomy with 1.25mm burr to orbital atherectomy for lesion modification. Right radial approach with 6Fr AL 0.75 guiding catheter was used but was difficult to deliver 1.5mm balloon or IVUS catheter distally. A Corsair Pro XS microcatheter was then placed in distal RCA to exchange out for a RotaFloppy guidewire. At this point, a "test" angiographic shot revealed significant Accordion phenomenon in mid RCA. We felt that rotational atherectomy through pseudo lesions which represent protruding folds of the vessel wall will confer a high risk of perforation. Our strategy changed at this point and decided for intravascular lithotripsy (IVL) instead. Using guide extension and Wiggle guidewire, we managed to progressively pre-dilate mid RCA with a semi-compliant 1.5mm balloon, non-compliant(NC) scoring 1.75mm balloon and NC 2.0mm balloon. A 3.5 x 12mm Shockwave balloon was used to deliver 80 pulses from mid to proximal RCA. Repeat IVUS showed "cracks" in the 360 arc of calcium. A drug-eluting stent 3.5 x 48mm was then deployed in proximal-mid RCA and post-dilated with NC 4.0mm balloon. Good final angiographic and IVUS results with no complications.
211101 - Accordion IVL - PCI 2-3 - Accordion effect with MC.Ser1.avi
211101 - Accordion IVL - PCI 2-5 - post IVL.Ser1.avi
211101 - Accordion IVL - PCI 2-8 - final RCA 1.Ser1.avi
Case Summary
It is important to conduct pre-PCI planning to ensure optimal lesion modification in a safe manner. When clinical situation changes such as the appearance of Accordion phenomenon, it is vital to recognize the potential issues and complications and change strategies accordingly. Intravascular lithotripsy shockwave therapy appears to be a safe and effective method for calcified lesion modification in Accordion phenomenon. Orbital and rotational atherectomy should be avoided in these cases.