
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-097
Coronary Perforation With a Twist
By Hoong Sheng Loh
Presenter
Hoong Sheng Loh
Authors
Hoong Sheng Loh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-097
CORONARY - Complications
Coronary Perforation With a Twist
Hoong Sheng Loh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
SBH
Relevant Clinical History and Physical Exam
61-year-old male with chronic smoking presented to a non-PCI capable center 36 hours after onset of chest pain during a Covid-19 pandemic lockdown. On arrival, he was having mild dyspnea but no more chest pain. Blood pressure was 110/68 mmHg, heart rate was 86/min, bibasal crepitations heard in the lungs, hearts sounds were unremarkable and no pedal edema. He was diagnosed with late presentation of STEMI and was transferred to a PCI-capable center on the next day.
Relevant Test Results Prior to Catheterization
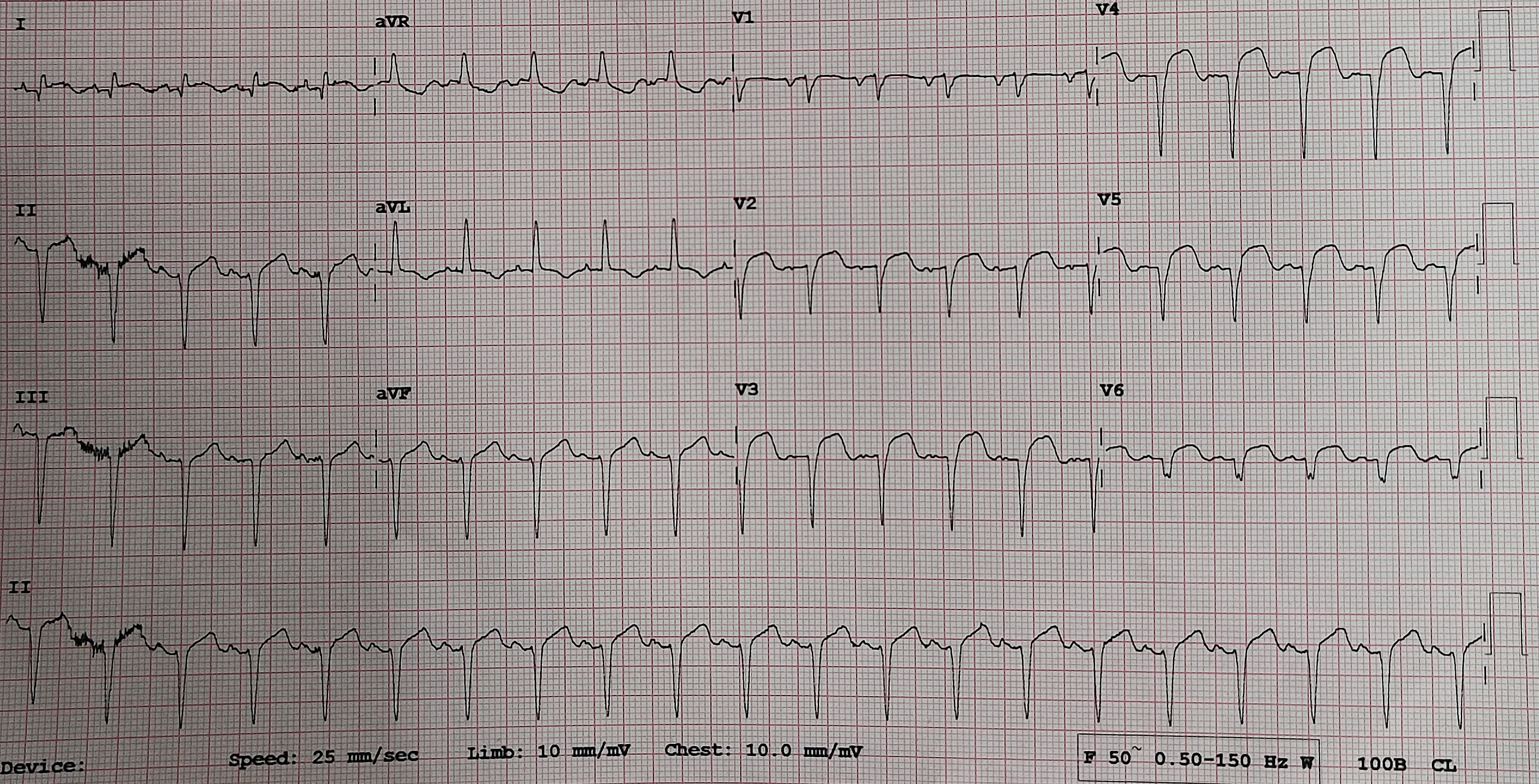
12-lead ECG showed ST-segment elevations in the anterolateral leads and extensive deep Q waves.
Relevant Catheterization Findings
Coronary angiogram showed normal left main stem, total occlusion from mid segment in the LAD, mild disease in the LCx and severe disease in the mid segment of RCA. The plan was PCI for LAD first and stage PCI for RCA later.
 Media1.mp4
Media1.mp4
Media2.mp4
Media3.mp4
Interventional Management
Procedural Step
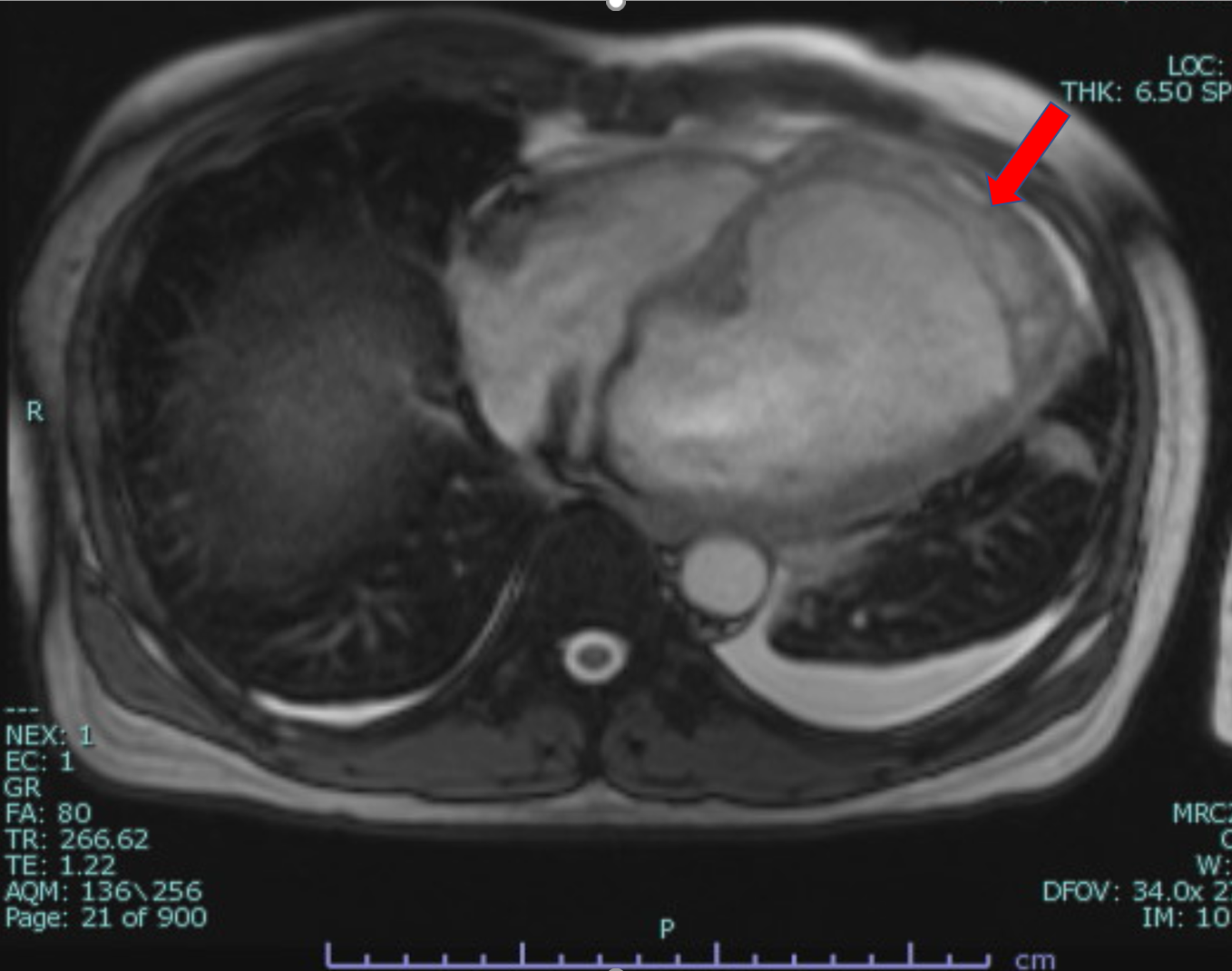
A Runthrough Floppy wire crossed the lesion but unable to pass into the distal LAD hence directed to a distal diagonal branch. Mid LAD was predilated with compliance balloon 2.5x15mm at nominal pressure and an extravasation was noted in the distal LAD suggestive of Ellis type 3 perforation. Patient was asymptomatic with mild hypotension. Echocardiogram showed akinetic mid-apical anterior wall with estimated EF 25% but no pericardial effusion seen. To prevent further hemodynamic deterioration, distal LAD was successfully sealed off with autologous fat embolization. He was stable after the procedure. Repeat echo showed dilated left ventricle with apical aneurysm and a dissecting intramyocardial hematoma in the mid-apical anterior wall, which was confirmed later with cardiac MRI. Repeat echo and cardiac MRI 3 weeks later showed significant size reduction of dissecting intramyocardial hematoma. Stage PCI to RCA was successfully performed and he was discharged without further complications.
Media4.mp4
Media5.mp4
Case Summary
Dissecting intramyocardial hematoma is a rare complication after an acute myocardial infarction that carries a high mortality rate. During the Covid-19 pandemic lockdown, we noted more patients were late in seeking medical attention after onset of myocardial infarction. This case demonstrated an acute dissecting intramyocardial hematoma immediately after predilatation of the occluded LAD for a patient with late presentation of myocardial infarction. Reocclusion of the LAD with fat embolization in this case had successfully prevented further progression of the dissecting intramyocardial hematoma and possible death.