
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-028
A Dilemma Between Mechanical Valve, Large Ischemic Stroke and Left Main Stent Thrombosis
By Wongwaris Aphijirawat
Presenter
Wongwaris Aphijirawat
Authors
Wongwaris Aphijirawat1
Affiliation
Queen Sirikit Naval Hospital, Thailand1,
View Study Report
TCTAP C-028
CORONARY - Bifurcation/Left Main Diseases and Intervention
A Dilemma Between Mechanical Valve, Large Ischemic Stroke and Left Main Stent Thrombosis
Wongwaris Aphijirawat1
Queen Sirikit Naval Hospital, Thailand1,
Clinical Information
Patient initials or Identifier Number
TJ
Relevant Clinical History and Physical Exam
Male 69-year-old with a history of severe AS s/p bileaflet mechanical AVR, HT, IHD s/p PCI 5 years ago(unknown status)Admit to stroke unit due to sudden Lt-sided hemiparesis for 1 hour PTA, rtPA was given.After hospitalization for 2 hours, he developed chest pain, hypotension and acute pulmonary edema. Intubation was required.He stopped warfarin for 1 month by himself.
V/s - BP 70/50 HR 60 RR 40 bpmHeart : valve click +veLung : crepitation bothNeuro : good consciousness, motor grade II Lt-sided
V/s - BP 70/50 HR 60 RR 40 bpmHeart : valve click +veLung : crepitation bothNeuro : good consciousness, motor grade II Lt-sided
Relevant Test Results Prior to Catheterization
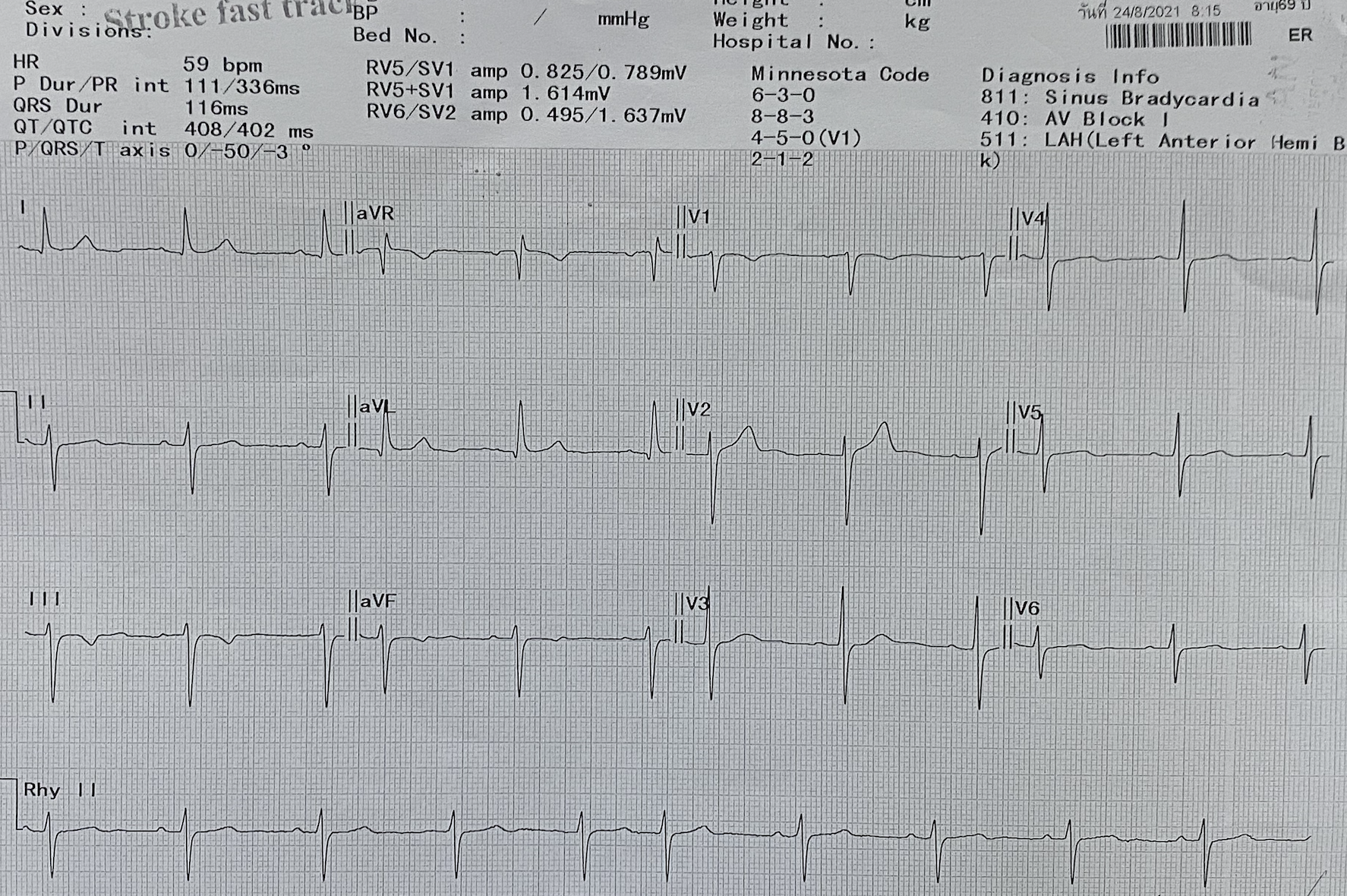
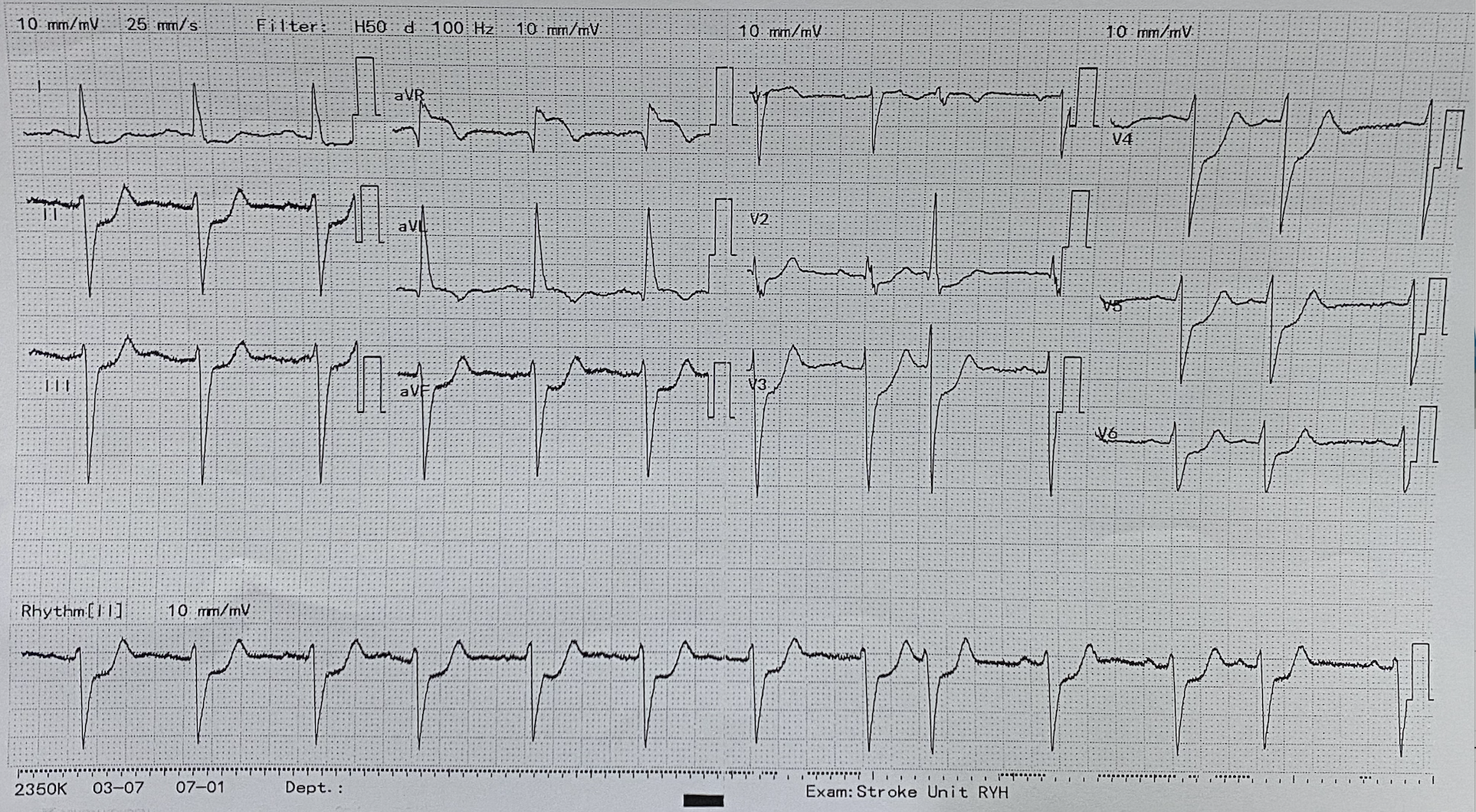
CT brain : Small acute infarction of Rt frontal lobe, no intracranial hemorrhageECG : NSR rate 60 bpm with diffuse ST depression in II, III, avF, V2-6 and ST elevation in avRCxR : Bilateral alveolar infiltration, sternal wire and mechanical aortic valveCBC : Hct 40% platelet 209,000, INR 1.02hsTnT : 6.8 (at stroke unit) -> 592 (after chest pain) -> 1630
Diagnosis : NSTEMI with acute heart failure and respiratory failure, cardiogenic shockAcute ischemic strokes/p Aortic mechanical prosthesis
Diagnosis : NSTEMI with acute heart failure and respiratory failure, cardiogenic shockAcute ischemic strokes/p Aortic mechanical prosthesis
Relevant Catheterization Findings
Left main : total occlusion of left main stent , LM stent protusion into aortaLAD : 70% stenosis at ostial to proximal segment.LCx : Non significant stenosis.RCA : Dominant vessel, non significant stenosis and give collateral flow to LAD and Lcx
Aortic bileaflet mechanical valve function - Normal leaflet movement
Imp : Suspected very late left main stent thrombosisNormal function of bileaflet AVR
 LAO Caudal.mp4
LAO Caudal.mp4
RAO Caudal.mp4
RCA LAO .mp4
RCA RAO .mp4
Aortic bileaflet mechanical valve function - Normal leaflet movement
Imp : Suspected very late left main stent thrombosisNormal function of bileaflet AVR
Interventional Management
Procedural Step
Discussion with neurologist, the chance of hemorrhagic transformation in this patient was very high due to large area of infarction.Anticoagulant shoud be postponed for at least 2 weeks. But at this time, patient was in cardiogenic shock. POBA to LM stent was planned for just open the flow.A 7F JL ST catheter was used.Workhorse (Runthrough, Whisper, Sion black) wires were unable to cross LM stent despite support of OTW balloon.Gaia first wire could pass the LM stent lesion into Lcx and confirmed via tip injection,1.5 x 20 and 2.5 x 15 mm SC balloons were predilate the lesion and IVUS showed neointimal hyperplasia and underexpansion of LM stent, LM diameter 5.0 mm5.0 x 8 mm NC balloon was dilate and restored TIMI III flow with 20% residual stenosis. Stenting was planned in the next 2 weeks.After PCI, patient could wean off ventilator in 3 days. Unfortunately, repeated CT brain 7 days later, hemorrhagic transformation was shown. DAPT and anticoagulant were discontinued for 1 month.Valve click was assessed everyday to assure the prosthetic valve function.1 month later, PCI to LM was performed. 7F EBU3.5 catheter, wiring to LAD+Lcx, repeated IVUS showed neointimal hyperplasia and wire was in proximal stent strut -> need to rewire again.Provisional stenting with 3.5 x 33 mm Firehawk stent was placed at LM-LAD, KBI and POT was done.Final angiogram and IVUS showed good result with TIMI III flow in the vessel. Warfarin + clopidogrel was given. Prosthetic valve, LM stent,no ICH
1st POBA - 2.5 SC dilate.mp4
1st POBA - 5.0 NC dilate-2.mp4
1st POBA - after 1.5 dilate.mp4
1st POBA - difficult OTW balloon delivery.mp4
1st POBA - final angio.mp4
1st POBA - tip injection.mp4
1st POBA 5.0 NC balloon.mp4
1st POBA final angio-2.mp4
1st POBA- 1.5 mm OTW dilate.mp4
1st POBA-final angio-3.mp4
2nd PCI - angio baseline.mp4
2nd PCI - final angio-3.mp4
2nd PCI - final angio-4.mp4
2nd PCI - KBI.mp4
2nd PCI - place stent.mp4
2nd PCI - POT 5.0 NC.mp4
2nd PCI - predilate.mp4
2nd PCI -angio baseline-2.mp4
2nd PCI -KBI-2.mp4
2nd PCI- final angio.mp4
2nd PCI-final angio-2.mp4
2nd PCI-place stent.mp4
IVUS postPCI.mp4
IVUS-prePCI.mp4
Case Summary
large ischemic stroke, ICH, prosthetic heart valve thrombosis and very late left main stent thrombosis in the same person produced a very complicated management. Timing of resume the medication is the critical thing. Timing of procedure, Simplest procedure step with less stent and IVUS usage looking for underly mechanism of stent failure needed to minimize the future ischemic and bleeding risks.