
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-072
Double Vessel Acute Myocardial Infarction With Extracorporeal Membrane Oxygenation(ECMO) Support
By Chin-Feng Tsai, Yao-Tsung Chuang
Presenter
Yao-Tsung Chuang
Authors
Chin-Feng Tsai1, Yao-Tsung Chuang1
Affiliation
Chung Shan Medical University Hospital, Taiwan1,
View Study Report
TCTAP C-072
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Double Vessel Acute Myocardial Infarction With Extracorporeal Membrane Oxygenation(ECMO) Support
Chin-Feng Tsai1, Yao-Tsung Chuang1
Chung Shan Medical University Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
MR.Yang
Relevant Clinical History and Physical Exam
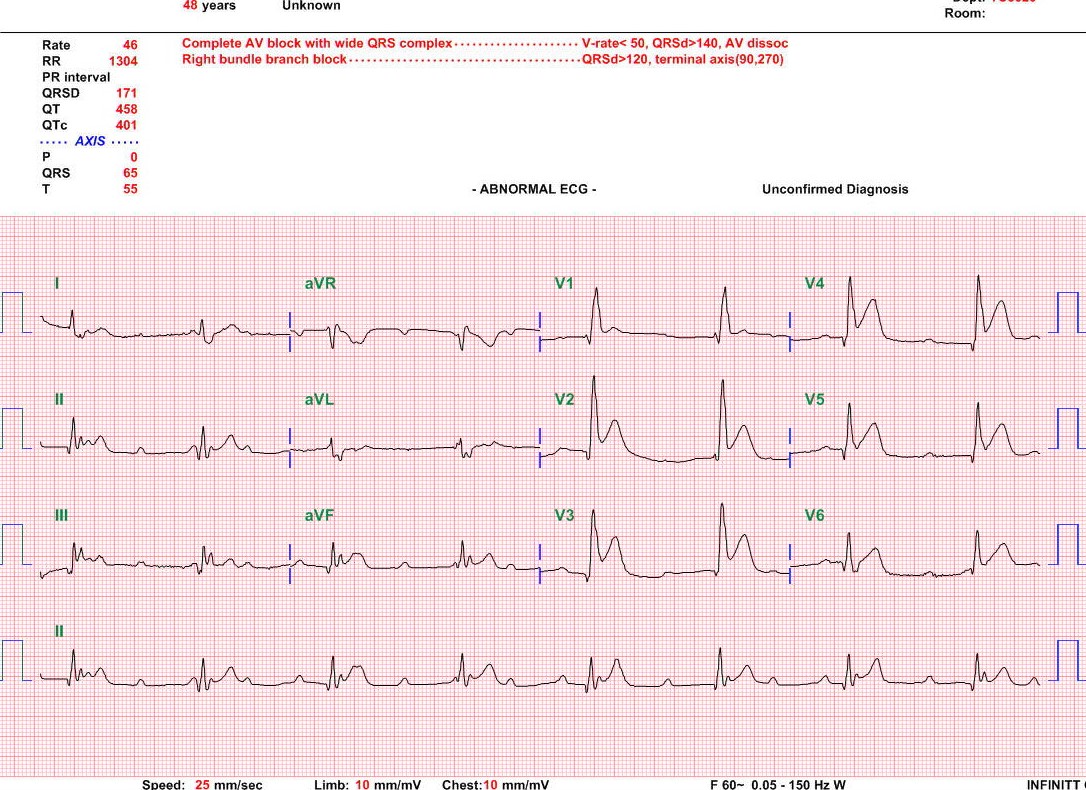
This 48-year-old man had Hypertension and hyperlipidemia. He smoked one pack per day for more than 30 years. He was brought to ER because of Chest pain with cold sweating and then syncope In the morning of admission day. When he arrived ER, He had cardiac collapse in ER; CPR was done.
ECMO support was done in ER. Then emergency PCI was arranged.
Relevant Test Results Prior to Catheterization
EKG revealed anterior wall STEMI and inferior wall STEMI; complete AV block was also noted.CXR revealed cardiomegaly and acute pulmonary edema.
Relevant Catheterization Findings
LM :patent
 CAG0.avi
CAG0.avi
CAG1.avi
CAG3.avi
CAG0.avi
CAG1.avi
CAG3.avi
Interventional Management
Procedural Step
Strategy :
PCI for LAD.mov
PCI for RCA.mov
Case Summary
This patient survival after percutaneous coronary intervention(PCI), under extracorporeal membrane oxygenator (ECMO) and intra-aortic balloon pump (IABP) support; EKG revealed sinus rhythm; Mean BP around 60-70 mmHg and consciousness alert about three days later; he can obey our order. We also prepared left ventricular assist device (LVAD) and heart transplantation for this patient. Unfortunately, patient expired 28 days later because of sepsis.
Conclusion:
Conclusion: