
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-082
One Moment Percutaneous Treatment of Heavily Calcific Subocclusive Left Main Stenosis and Triple Coronary Artery Disease with Concomitant Severe Aortic Stenosis: Valvuloplasty for Impella Implantation and All Stenosis Treatment
By Bernardo Cortese, Elisabetta Iardino, Gaetano Di Palma, Farhat Fouladvand
Presenter
Farhat Fouladvand
Authors
Bernardo Cortese1, Elisabetta Iardino2, Gaetano Di Palma1, Farhat Fouladvand1
Affiliation
Clinica San Carlo, Italy1, Ospedale Bolognini, Italy2,
View Study Report
TCTAP C-082
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
One Moment Percutaneous Treatment of Heavily Calcific Subocclusive Left Main Stenosis and Triple Coronary Artery Disease with Concomitant Severe Aortic Stenosis: Valvuloplasty for Impella Implantation and All Stenosis Treatment
Bernardo Cortese1, Elisabetta Iardino2, Gaetano Di Palma1, Farhat Fouladvand1
Clinica San Carlo, Italy1, Ospedale Bolognini, Italy2,
Clinical Information
Patient initials or Identifier Number
CE 16/04/1941
Relevant Clinical History and Physical Exam
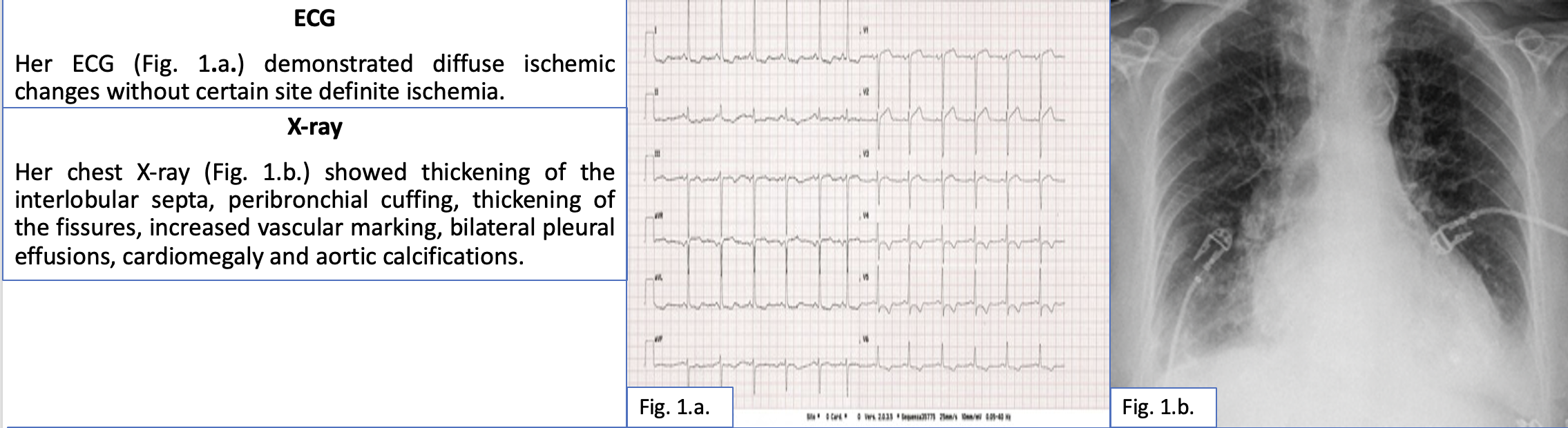
A 80 years of age lady without any previous disease were conducted to our emergency department due to dyspnoea lasting several hours. At arrival in our emergency department the patient was still dyspnoeic. Her ECG demonstrated diffuse ischemic changes without certain site definite ischemia. Her chest X-ray showed thickening of the interlobular septa, peri-bronchial cuffing, thickening of the fissures, increased vascular marking, bilateral pleural effusions, cardiomegaly and aortic calcifications.
Relevant Test Results Prior to Catheterization
Her laboratory data revealed increase in myocardial necrosis markers as her TnI-HS was 3450 ng/ml and relatively normal values of other parameters.
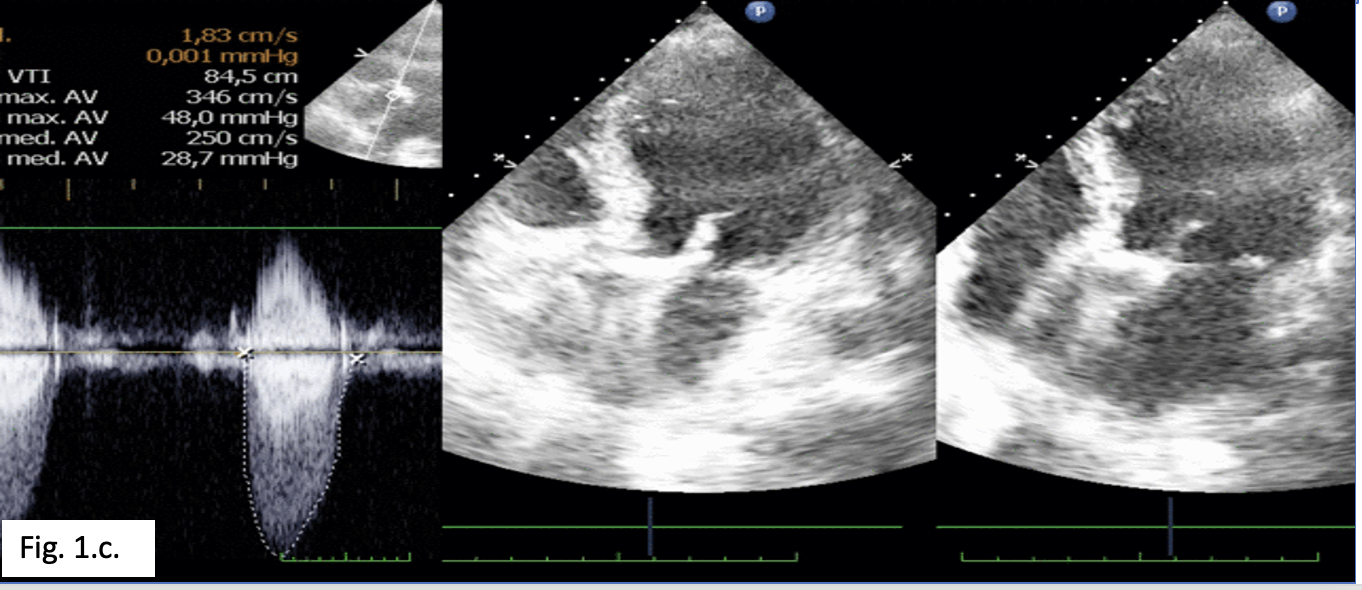
At echocardiography flash we found severe aortic valve calcification causing stenosis with peak gradient 48 mmHg, mean gradient 28 mmHg and diffuse segmental hypokinesis of left ventricle with global systolic function about 30%.
The DAPT was started and the patient was planned for coronary angiography within 24 hours of admission.
Relevant Catheterization Findings
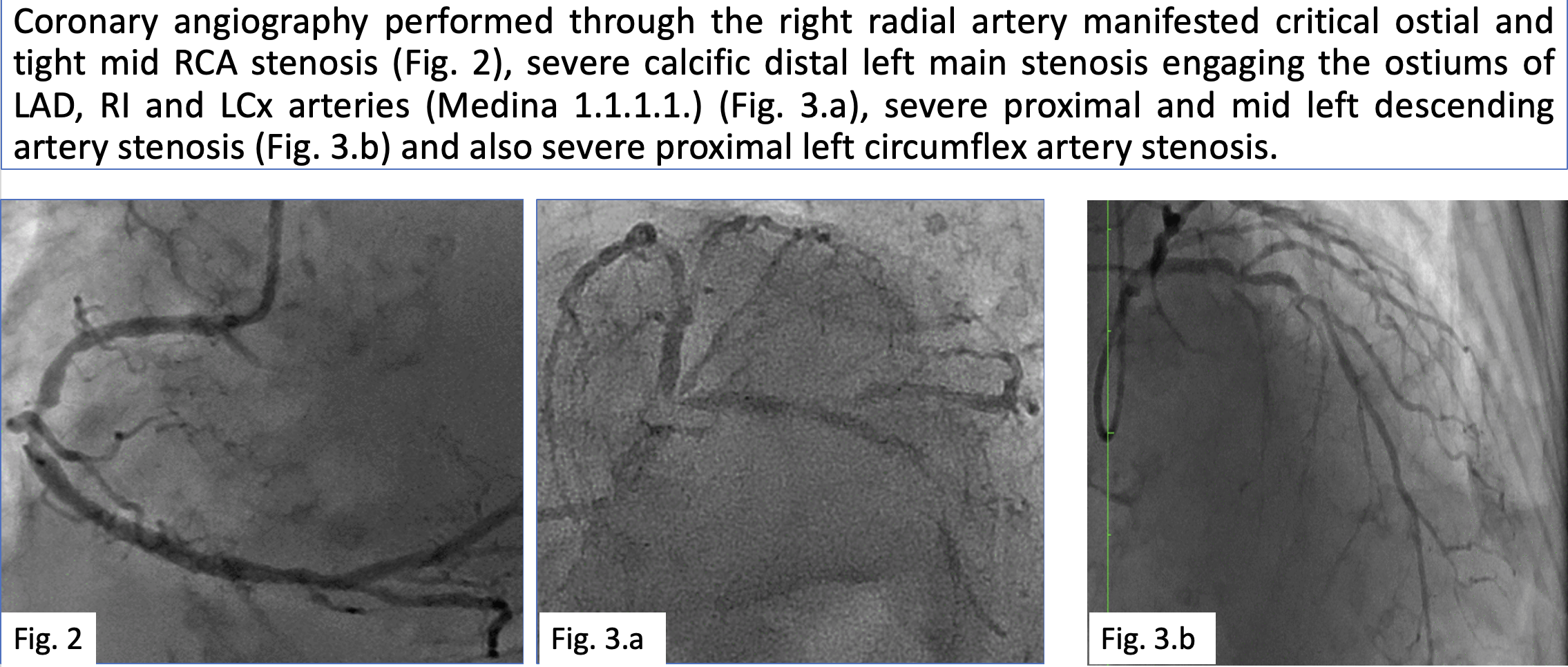
Coronary angiography performed through the right radial artery shoed ostial and mid RCA stenosis, severe calcific distal left main (Medina 1.1.1.), mid LAD and mid Lcx stenosis (Fig.3). At the time of COVID any transfer to any surgical center was extremely difficult so after discussion with the patient and the family we fixed the RCA with one in the mid segment and one ostial DES. Then after aortic valvuloplasty (Valver 20 mm) for Impella 2,5 placement in the left ventricle was done.
Interventional Management
Procedural Step
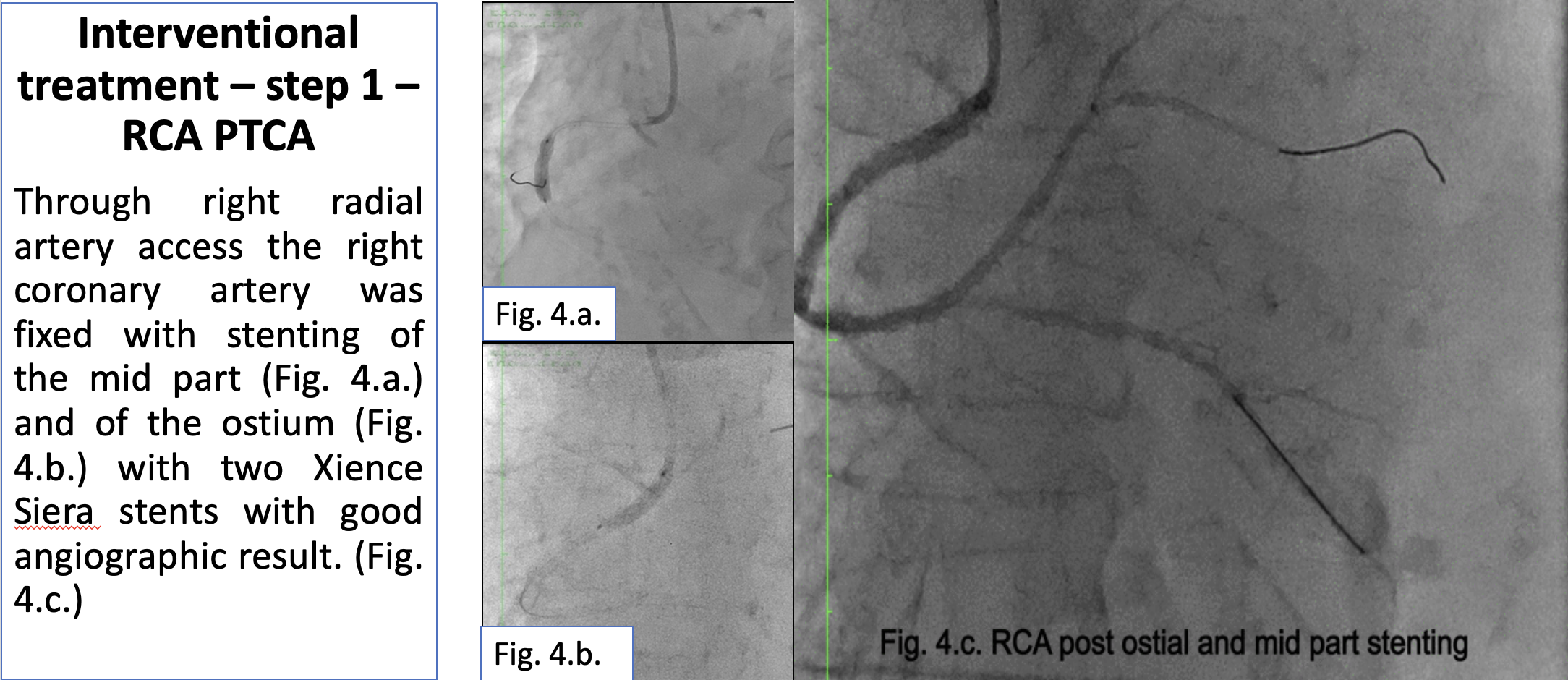
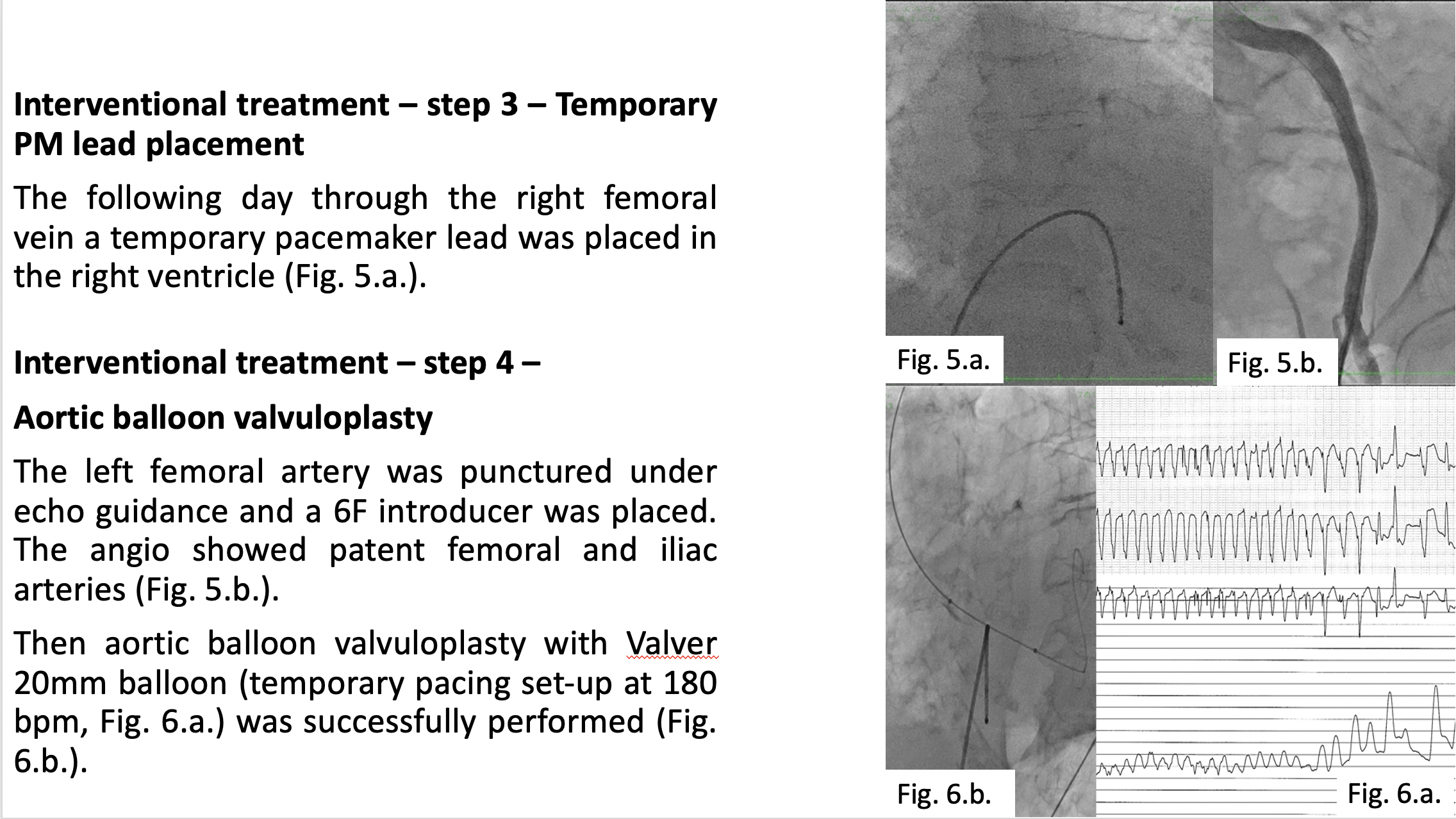
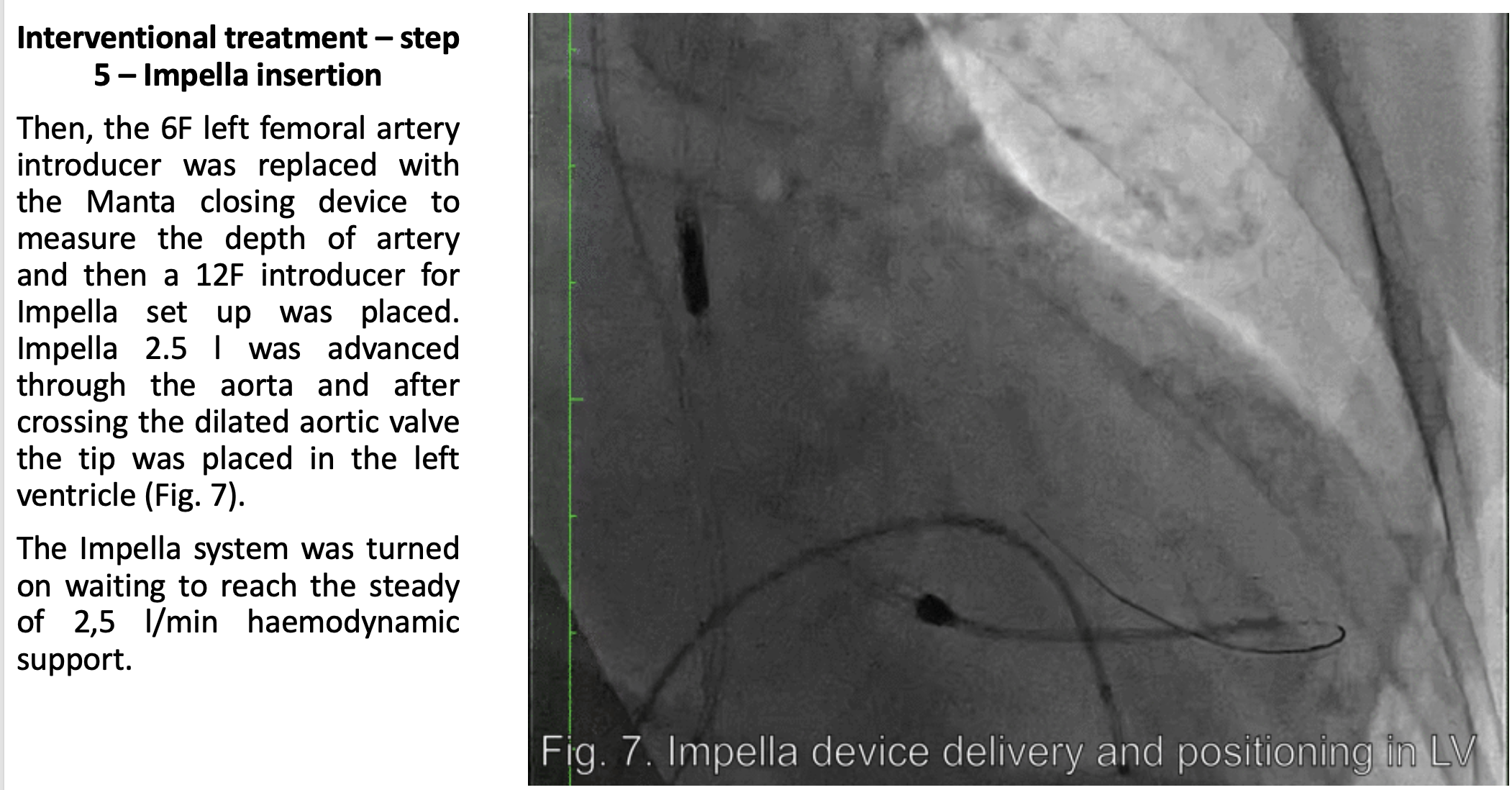
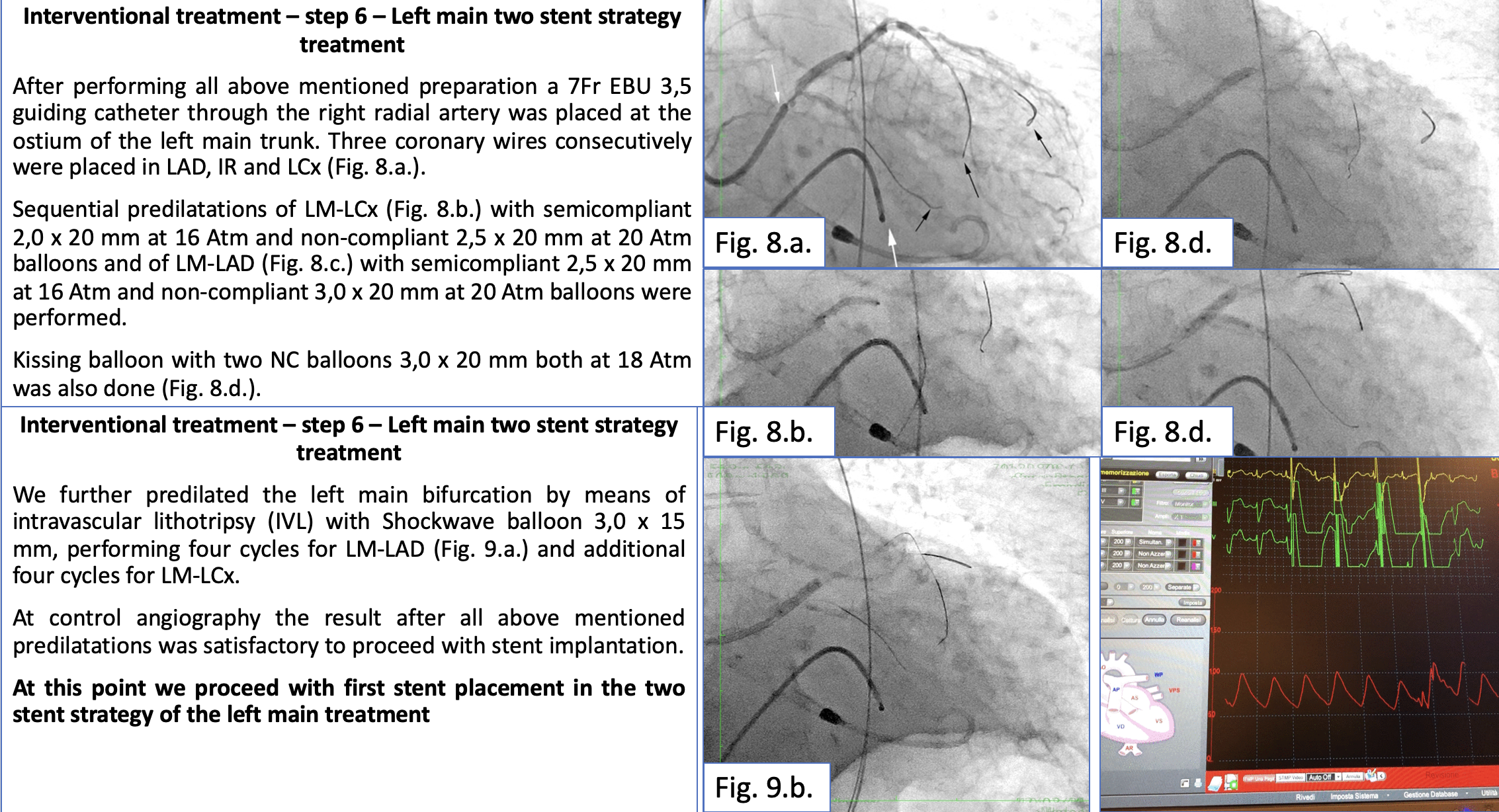
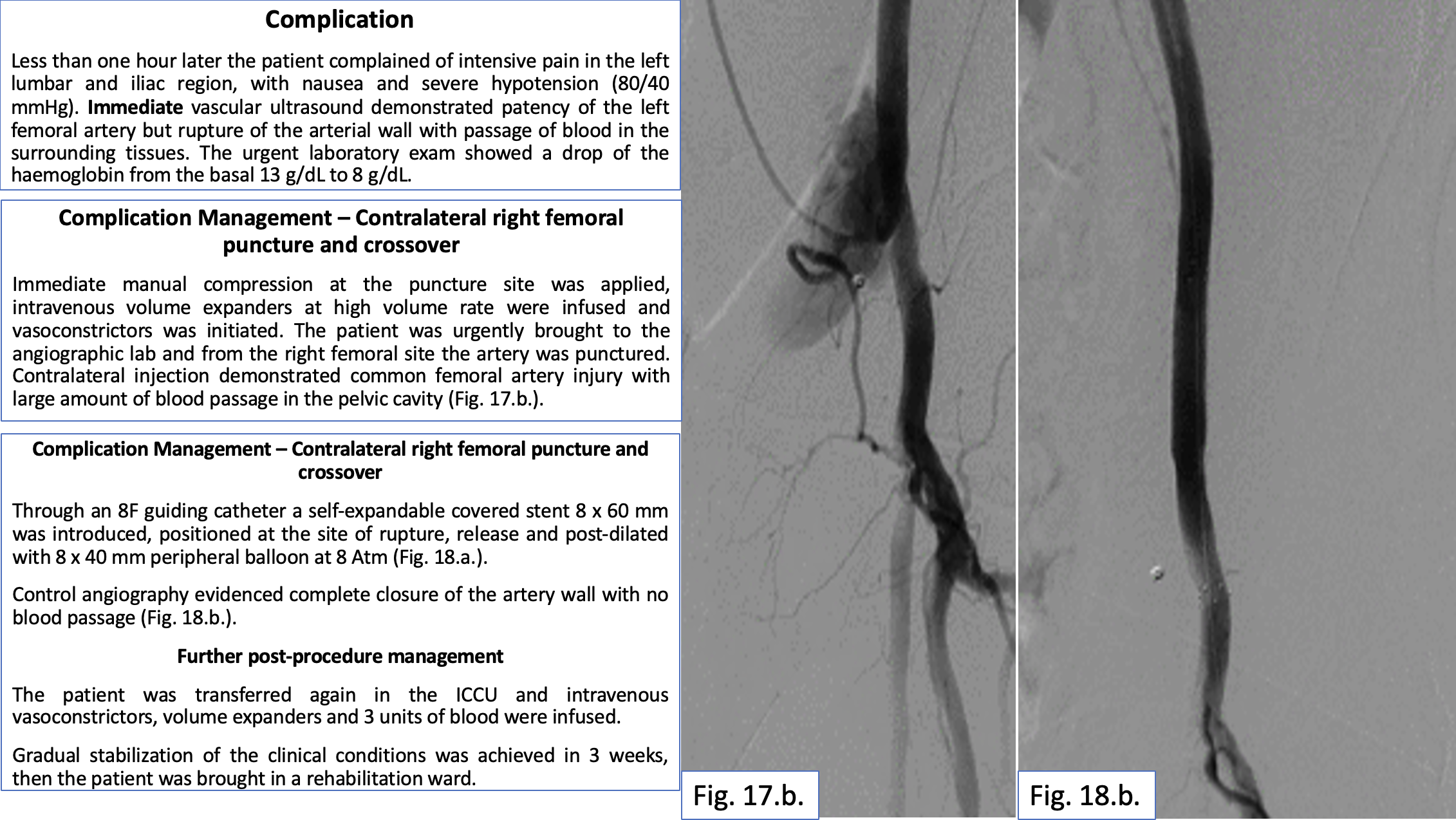
Through right radial artery access the right coronary artery was fixt with stenting. Then aortic balloon valvuloplasty (Valve 20 mm). The Impella device was advanced and after crossing the dilated aortic valve the tip was placed in the left ventricle. Sequential predilatations of LM-LAD and LM-LCx with semicompliant, non-compliant and scoring balloons were performed. For persisting of unacceptable for stenting result we continued the preparation of LM bifurcation with predilatation using intravascular lithotripsy (IVL) with Shockwave balloon on LM-LAD and LM-CX. Then we implanted one bifurcation dedicated stent Bioss Lim on the axis LM-LCx. After predilatation of mid LAD we placed one drug eluting stent from LM to LAD proximal through the Bioss stent (short culotte stenting). The procedure was ended with drug coated balloon on LAD mid and with drug coated balloon inflation on LCx mid. Then Impella was removed and vascular closure was achieved with Manta closing device. In the ICCU the patient complained of intensive pain in the left lumbar and iliac region, nausea and severe hypotension (80/40 mmHg blood pressure). Contralateral injection demonstrated common femoral artery injury with large amount of blood passage in the pelvic cavity. A self-expandable covered stent 8 x 60 mm was introduced and placed at the site of artery rupture.
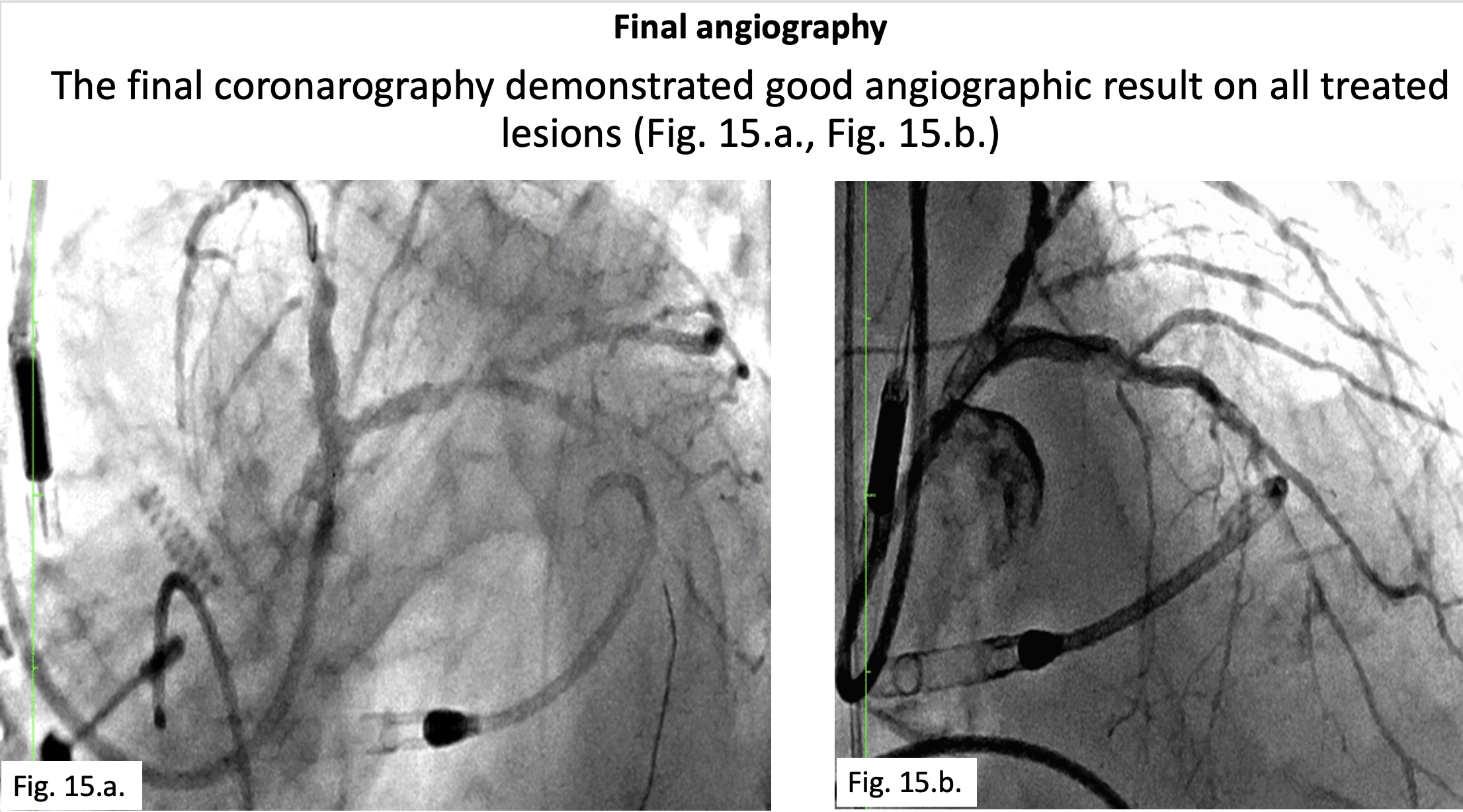
The control angiography evidenced complete closure of the artery wall with no blood passage.
Case Summary
In time of pandemic restrictions decision of treatment must be done using available in-hospital facilities. The presence of aortic valve stenosis and multi-vessel disease and low ejection fraction requires contemporary preparation of aortic valve for haemodynamic support during coronary angioplasty. Vessel preparation can be achieved with new devices as intravascular lithotripsy (IVL) to reduce the risk of complication. DCB are valid alternative to DES particularly in small vessels with long atherosclerotic disease. Vascular access site dramatic complications in the experienced hands and well-organized catheterization laboratory can be managed withing the cathlab percutaneously.