
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-068
An Alternative Treatment Strategy for Graft Failure in ST-elevation Myocardial Infarction
By Wei-Jung Lo, Chih Hung Lai
Presenter
Wei-Jung Lo
Authors
Wei-Jung Lo1, Chih Hung Lai1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-068
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
An Alternative Treatment Strategy for Graft Failure in ST-elevation Myocardial Infarction
Wei-Jung Lo1, Chih Hung Lai1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
000464015H
Relevant Clinical History and Physical Exam
A 68-year-old man had a history of : (1) triple-vessel coronary artery disease (CAD), s/p coronary artery bypass graft (CABG) (Ao-SVG-LAD; Ao-SVG-int.OM-PDA) in 2005/11; (2) diabetes; (3) hyperlipidemia. This time, he suffered from chest tightness, and cold sweating in early morning on 2021/05/08 and he came to our hospital with diagnosis of inferior wall ST-elevation myocardial infarction (STEMI).
Relevant Test Results Prior to Catheterization
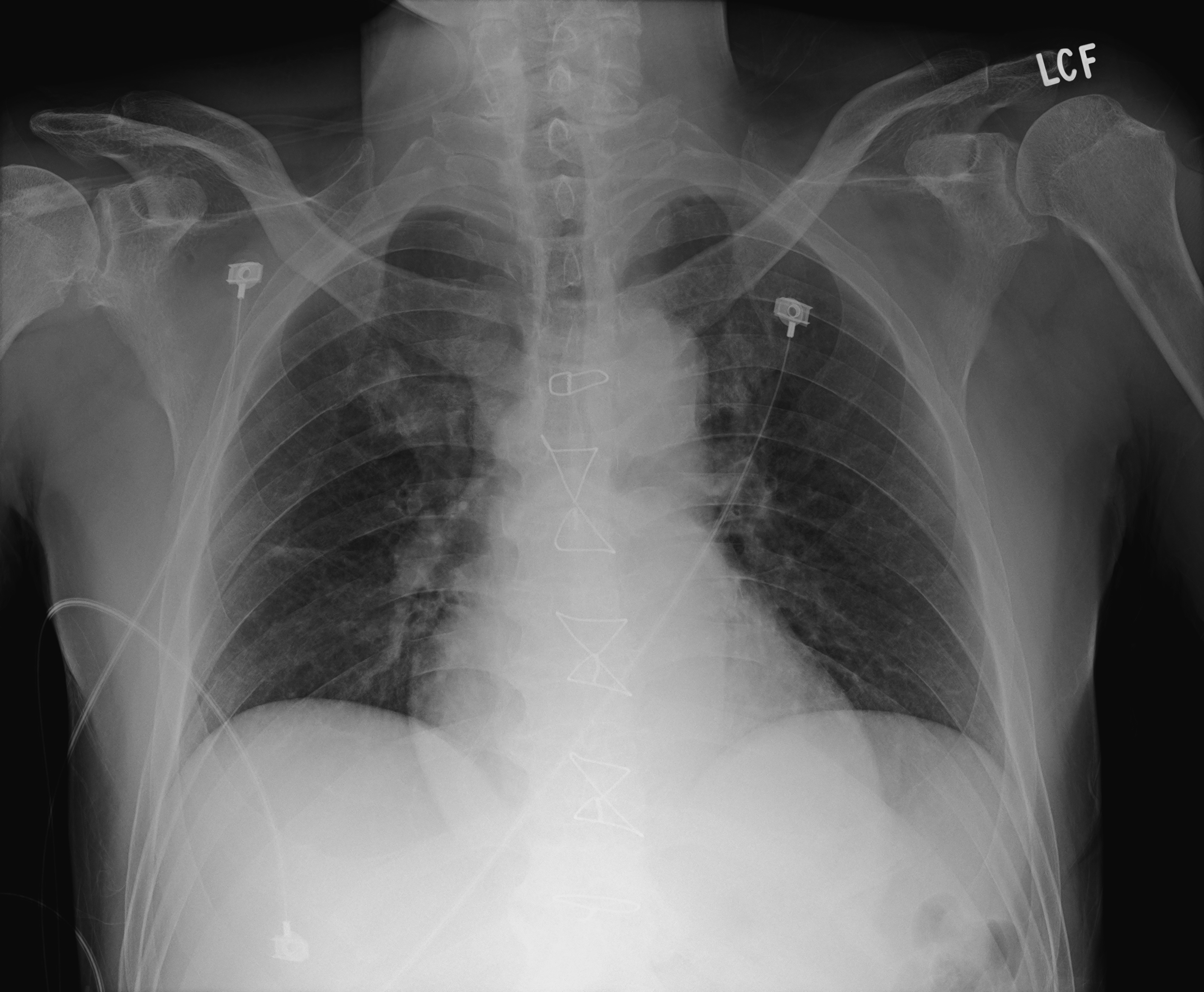
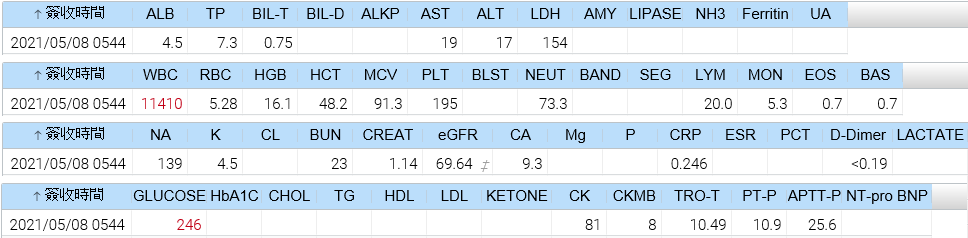
EKG : ST segment elevation over lead II, III and aVF with reciprocal change over lead I, aVL and V2~V4Chest x-ray : no obvious lung lesion, or pulmonary edema Laboratory study : no significant findings

Relevant Catheterization Findings
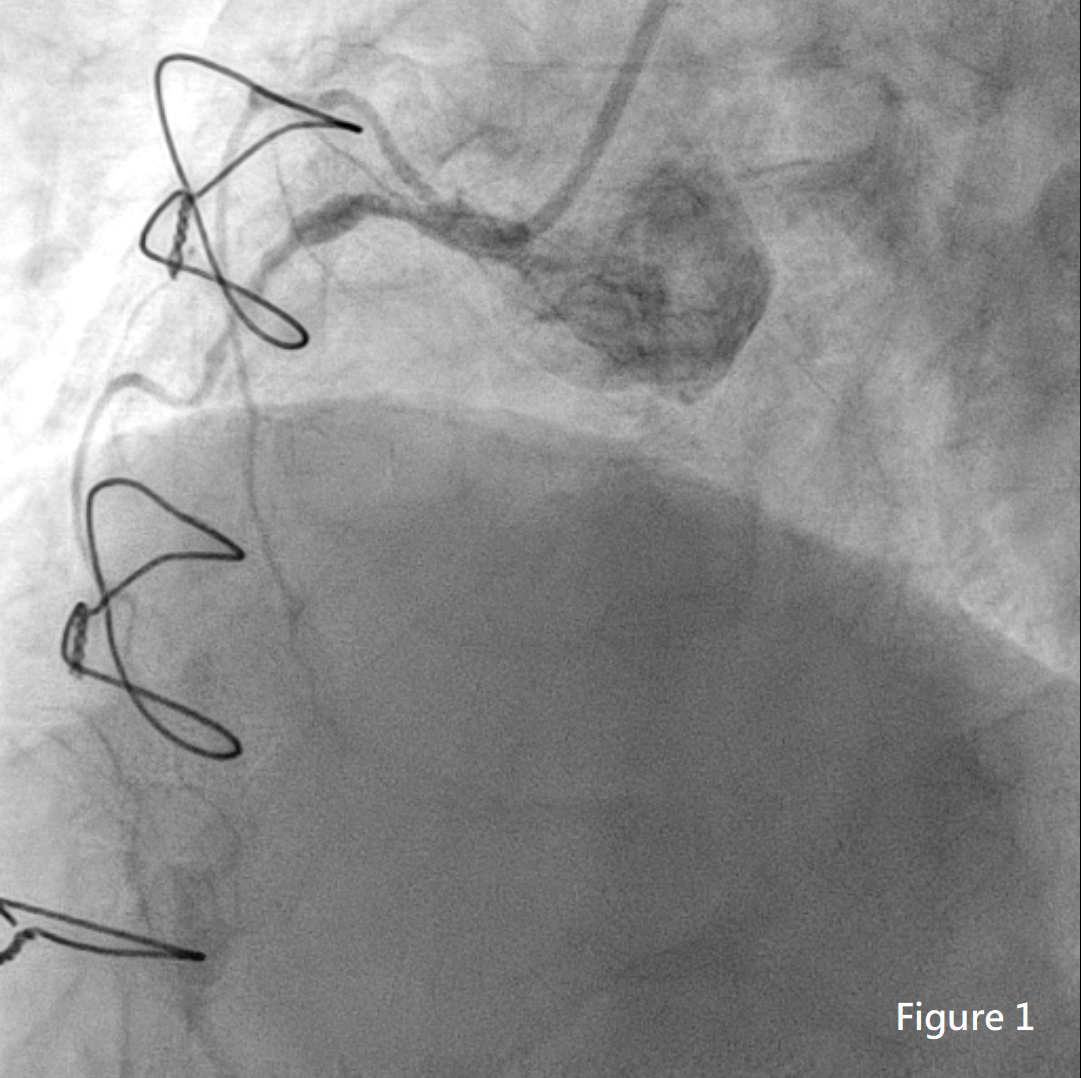
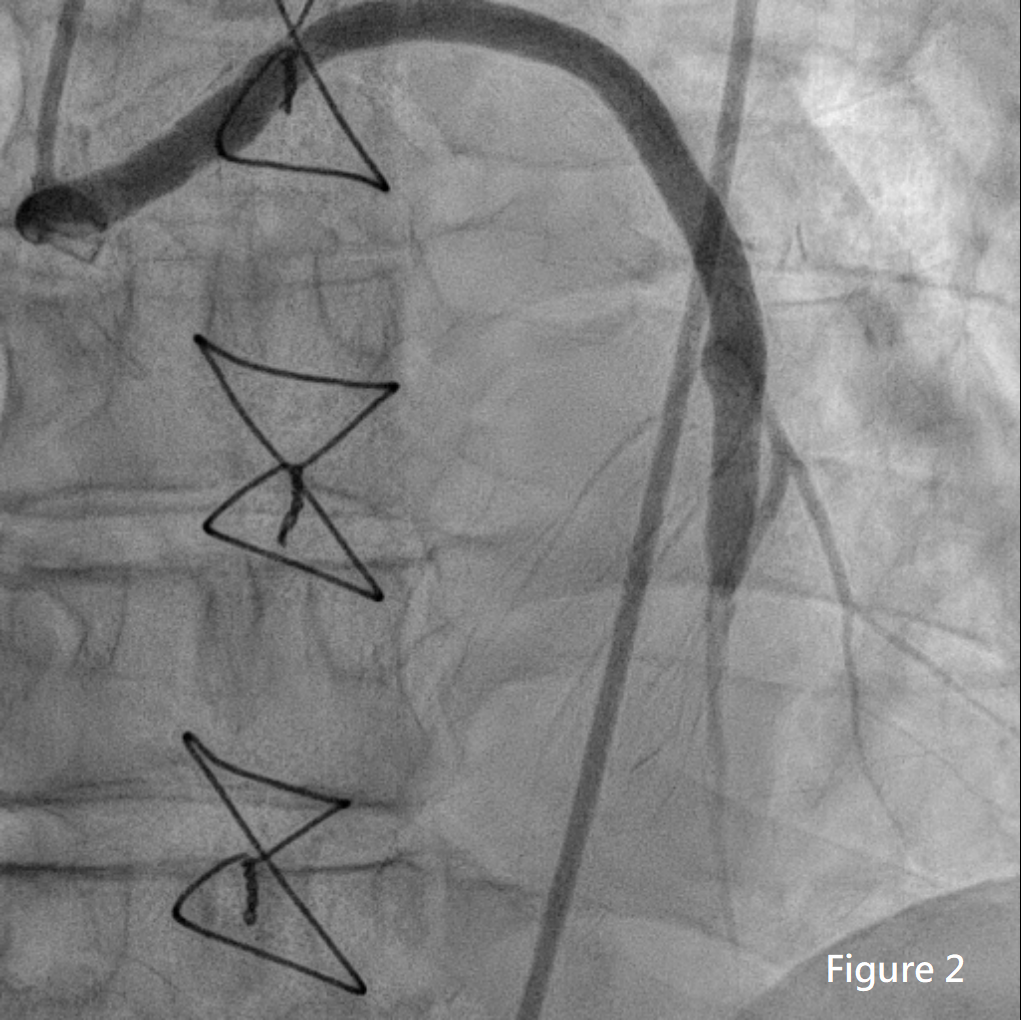
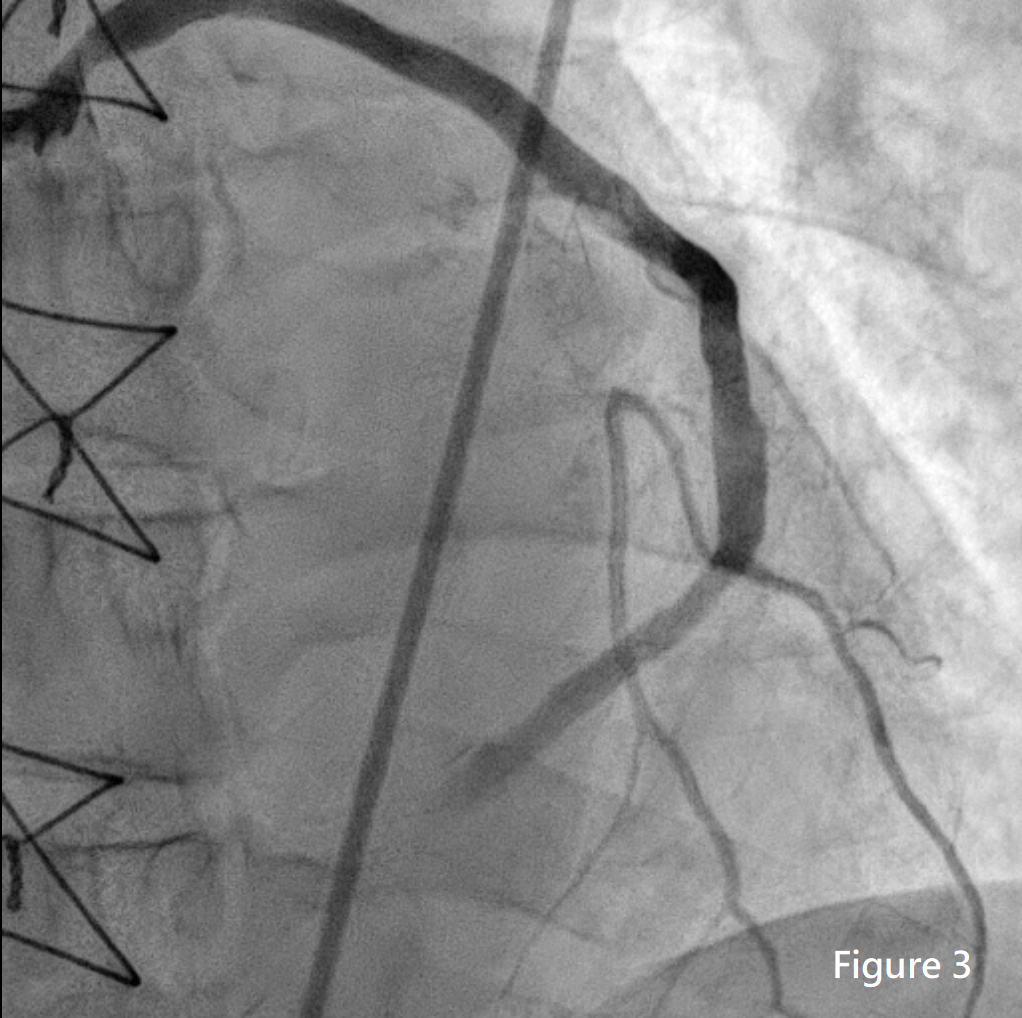
Coronary angiography (CAG) showed severe stenosis up to 80-90% of proximal right coronary artery (RCA) and total occlusion of middle RCA (Figure 1); Great saphenous vein (GSV) to left anterior descending artery (LAD) was patent (Figure 2); GSV to obtuse marginal (OM) of left circumflex artery (LCX) was patent; total occlusion of LCX-OM to RCA-PDA (Figure 3).
Interventional Management
Procedural Step
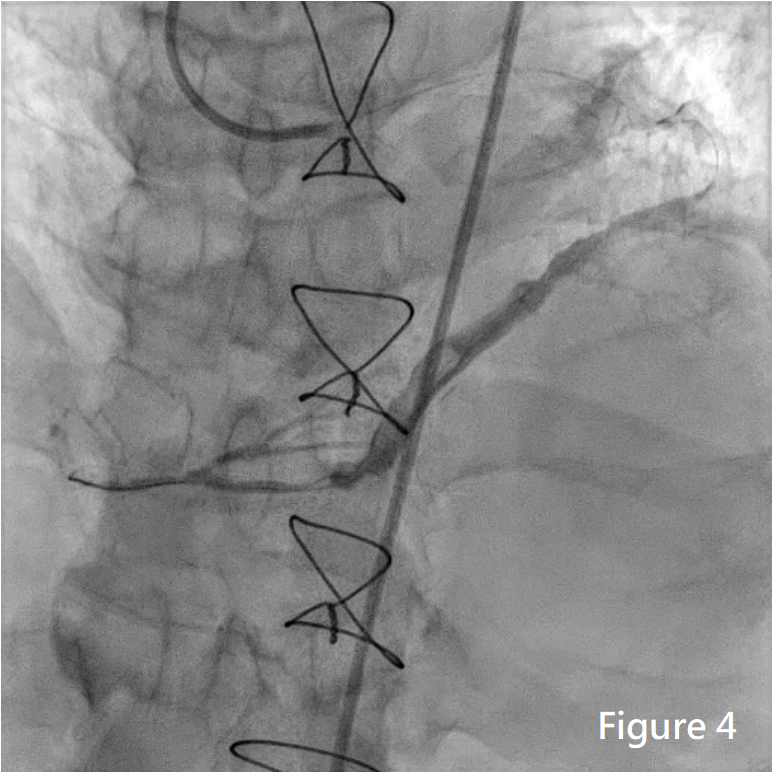
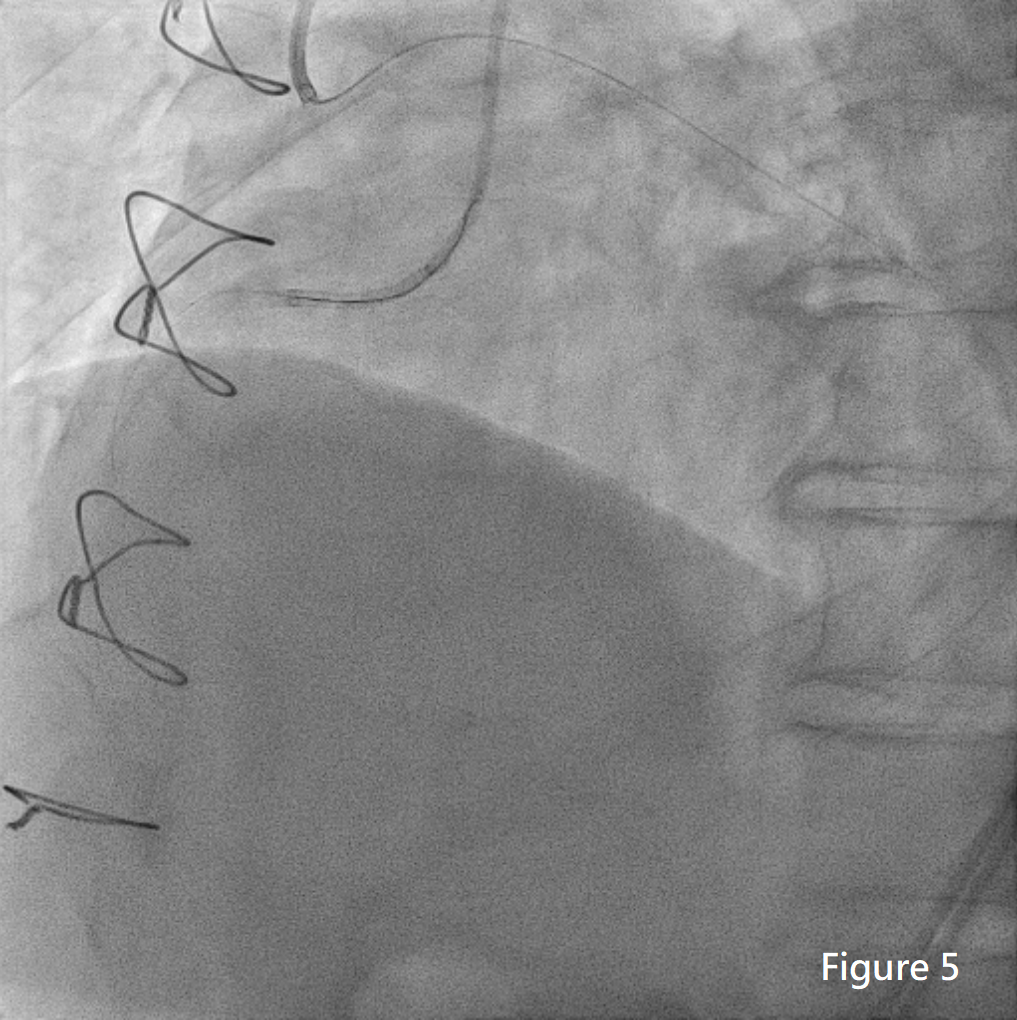
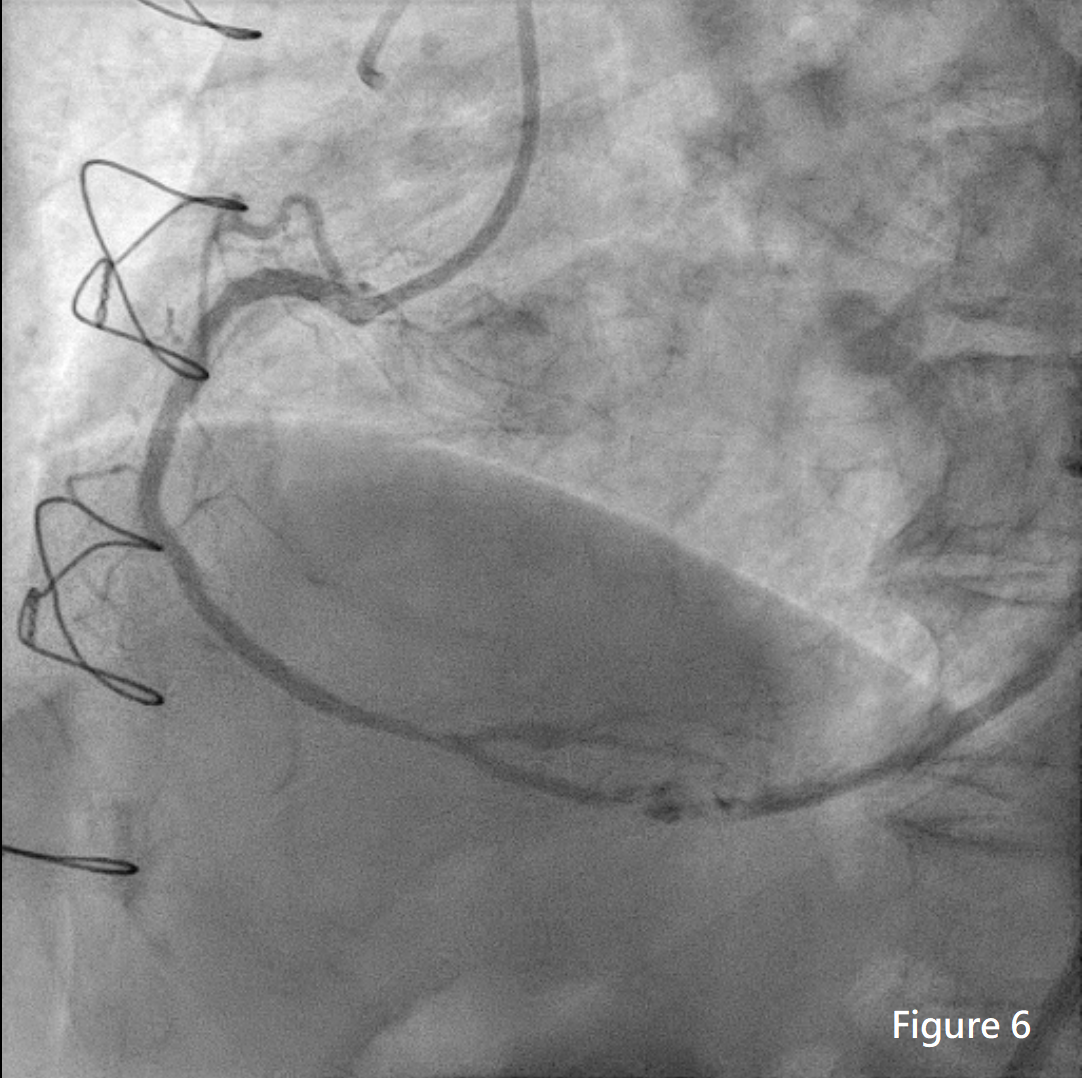
SAL guiding catheter was engaged to RCA. With APT microcatheter, Fielder FC guidewire and Fielder XTA GW could not cross the total occlusion. Then SAL was engaged to GSV. With APT microcatheter, Fielder FC was advanced to RCA-D successfully. We did thrombus suction with Eliminator. Then huge thrombus over distal GSV and critical stenosis over GSV to PDA junction were noted. We did dilation with balloon catheter and intracoronary Aggrastat infusion. The flow became to TIMI II. However, severe recoil stenosis and huge thrombus persisted (Figure 4). We did RCA intervention in case of poor flow of thrombotic GSV. SAL was engaged to RCA. The retrograde Gaia 2 GW wasadvanced to RCA-M. With distal GW guiding, the antegrade Gaia 3 GW was advanced to RCA-D successfully. However, APT microcatheter could not cross the CTO. With GuideLiner, RCA-D was sequentially dilated by small BC. During retiring BC, Gaia 3 was pulled out due to impingement of GW and BC. We tried antegrade approach back with Fielder XTR GW but failed. We shifted to retrograde approach with Fielder FC and it could advanced into antegrade GC (Figure 5). Then we did retrograde Rendezvous technique and antegrade APT microcatheter was advanced to RCA-PDA through retrograde GW successfully. The antegrade ATP was replaced with Sion blue GW. The proximal to distal RCA was dilated with BC. Three Resolute Onyx DES were deployed at ostium to distal RCA. After POT, the final angiography of RCA showed TIMI III flow, even to RCA-GSV (Figure 6).
Case Summary
Here we present a case of graft failure which caused ST-elevation myocardial infarction. It is essential to understand the characteristics of vein graft. Acute occlusion of GSV is commonly associated with extensive atherosclerotic and thrombotic burden, which increased the risk of distal embolization and no-reflow and, thus, death and myocardial infarction. Preferential intervention of the native coronary arterial circulation should be considered as an alternative route to make reperfusion of the myocardium and, if possible, will result in higher acute success and late patency rate.