
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-091
A Case of No-Reflow due to Under Expansion of the Stent
By Amjad Ali, Dileep Kumar Tiwari
Presenter
Amjad Ali
Authors
Amjad Ali1, Dileep Kumar Tiwari2
Affiliation
Sagar Multispeciality Hospital, India1, Baderiya Metroprime Hospital, India2,
View Study Report
TCTAP C-091
CORONARY - Complications
A Case of No-Reflow due to Under Expansion of the Stent
Amjad Ali1, Dileep Kumar Tiwari2
Sagar Multispeciality Hospital, India1, Baderiya Metroprime Hospital, India2,
Clinical Information
Patient initials or Identifier Number
MM
Relevant Clinical History and Physical Exam
A70-year-old male with hypertension, diabetes, dyslipidemia, and an activesmoker presented to our emergency department with a worsening of angina of twodays' duration. He was a known case of ischemic heart disease andunderwent PTCA to LAD two years ago and had angina on exertion for 3 months. Hewas hemodynamically stable; his BP was 130/70 and his heart rate was 90 beatsper minute. He was taking low-dose aspirin, rosuvastatin, beta-blockers,long-acting nitrates, and nicorandil.
Relevant Test Results Prior to Catheterization
His electrocardiogram revealed sinus rhythm with leftbundle branch block, and a 2D echocardiogram showed mild global left ventriclehypokinesia with an ejection fraction of 50%. His troponin I was within thenormal range. We planned to do a coronary angiogram and, if required, furtherrevascularization.
Relevant Catheterization Findings
Acoronary angiogram was done via the right femoral artery. Angiography showed apatent LAD stent with TIMI III flow in the distal LAD. The LCX remained as themajor OM, with proximal critical 90–95% stenosis and calcification, while thedistal LCX was occluded, which was filled via collaterals and appears to besmall in diameter. RCA was a dominant vessel and showed mild luminalirregularities with no flow-limiting lesions.
 1.avi
1.avi
6.avi
Interventional Management
Procedural Step
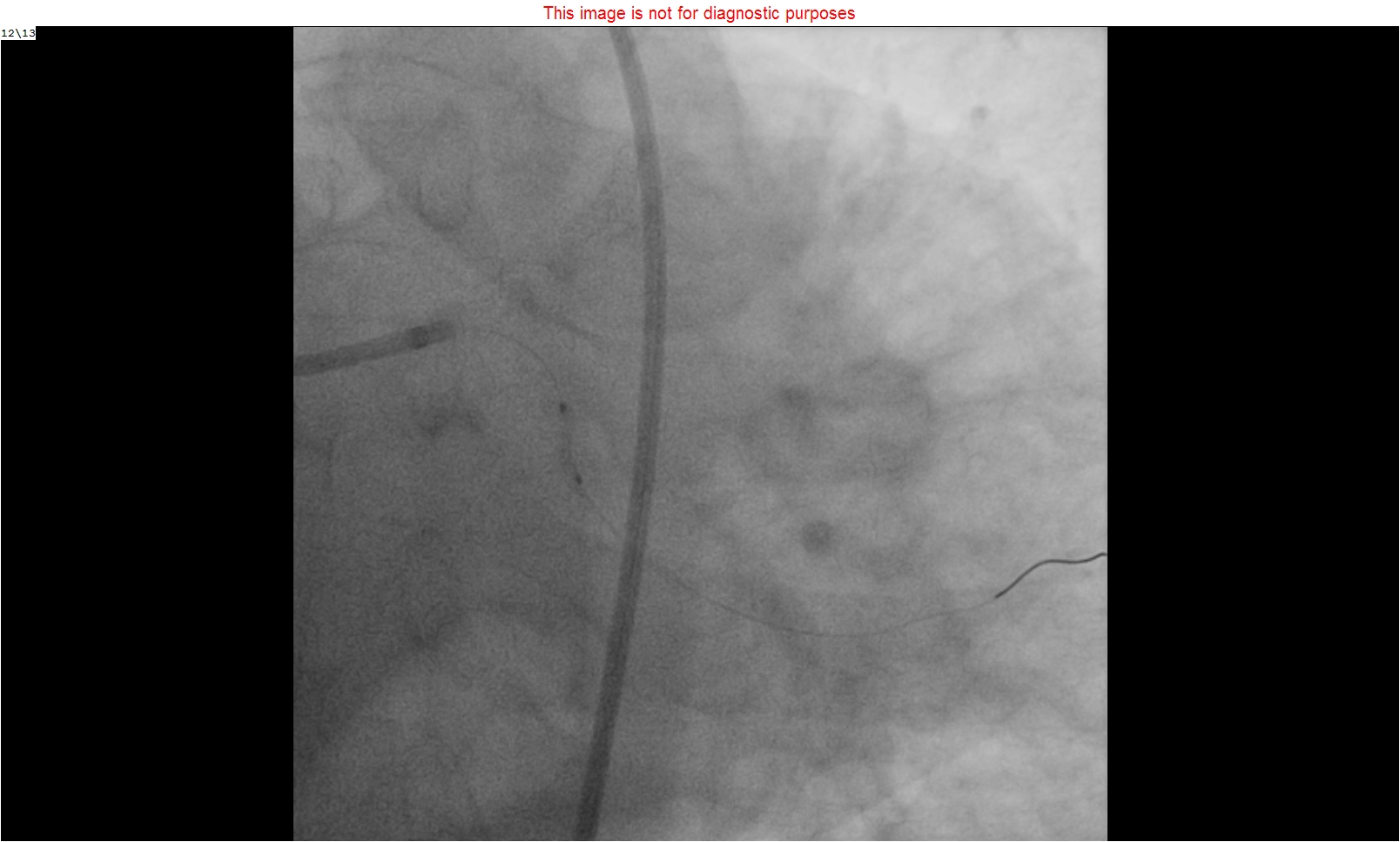
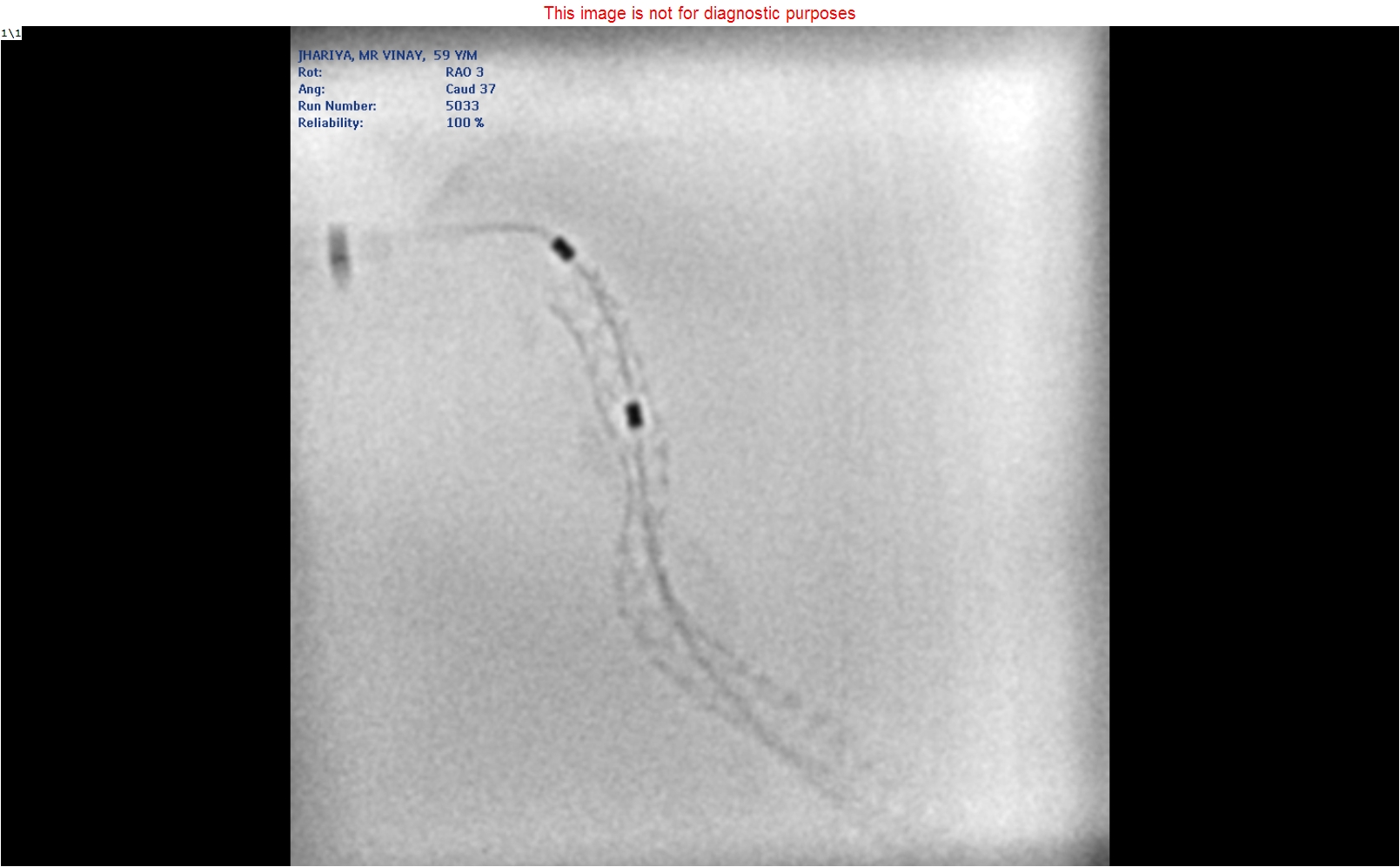
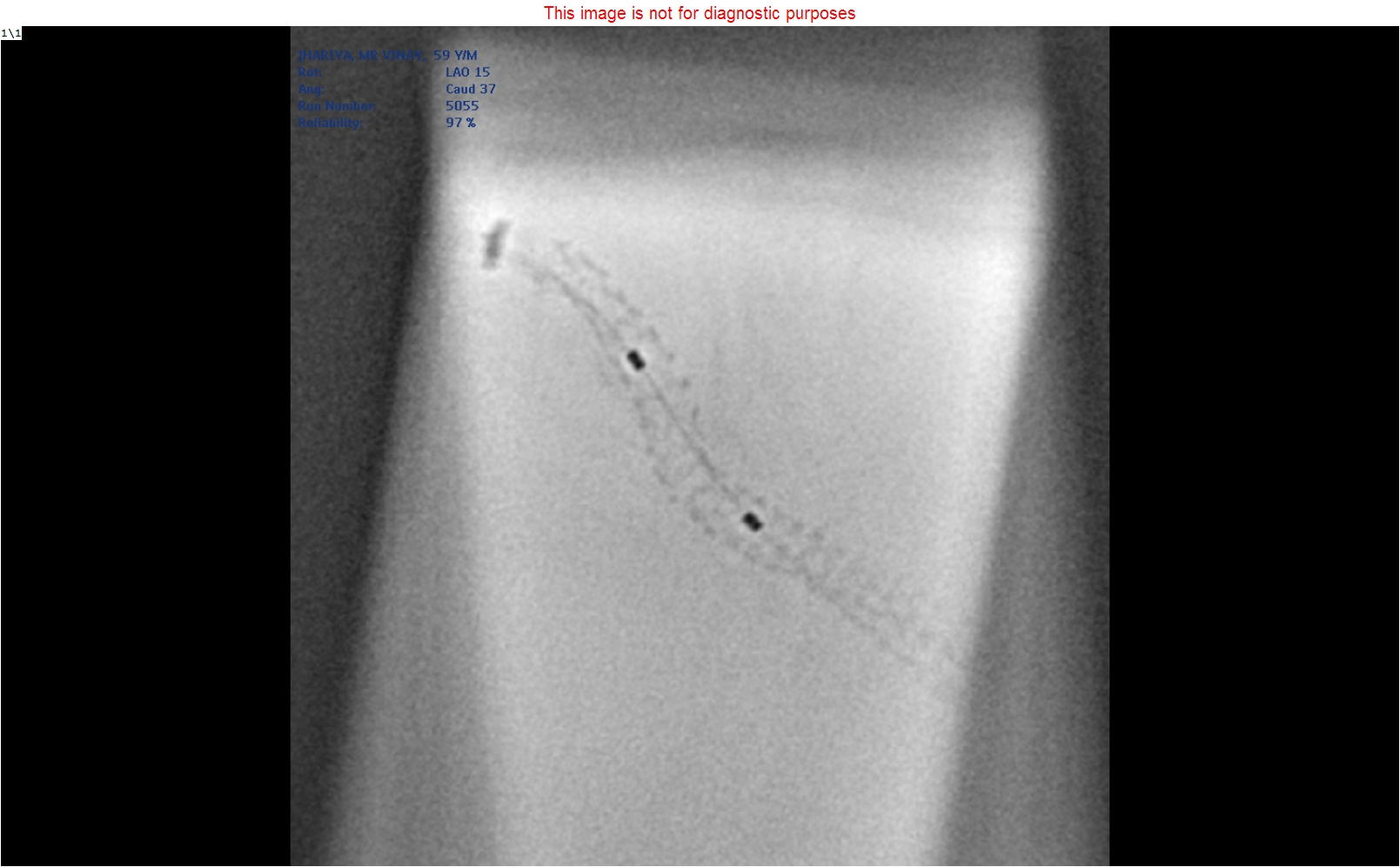
We planned to do angioplasty of the proximal LCX.After crossing the lesion by workhorse guidewire, the lesion was predilatedserially by a 1.5x10 semi-compliant balloon, followed by a 2x10 non-compliantballoon with high-pressure inflation. A 2.25x23 drug-eluting stent was deployedacross the lesion with nominal pressure. After stent deployment, an angiogramshoot showed good flow in major OM. Then we planned to do post-dilatation ofthe stent with a 2.25x10 non-compliant balloon, which was not crossing throughthe stent, so we took a stent boost, which surprisingly revealed severelyunder-expanded stent. It was tried to post dilate with several balloons, buteven a 1.0 mm balloon was not crossing the under expended part of the stent. Wetried to exchange the wire with an extra-stiff guidewire, but the microcatheterwas also not crossing that segment. During the procedure, the patient hadsevere chest pain. The monitor showed ST elevation, and the angiogram shootshowed no-reflow in major OM. Then we tried to cross the stent directly with anextra stiff Allstar (Abbott) guidewire, and fortunately that guidewire crossedthe stent. First, we passed a 1.25x8 mm balloon, followed by 1.5x10, 2x10, andfinally a 2.5x10 non-compliant balloon, and did post dilatation byhigh-pressure inflation. The final shot showed a well-expanded stent with TIMIIII flow in the distal vessel.
final shoot.avi
Case Summary
Stent under expansion is usually defined as thefailure to achieve a minimal in-stent dimension of more than 80% of the averagereference segment diameter in patients with PCI. Under-expanded stents can leadto acute vessel closure and the need for stepwise post-dilatation by using thesmaller diameter of non-complaint balloons. Extra stiff guidewires will provideadditional support for non-compliant balloons crossing across the underexpanded stents, as in our case.