
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-165
Real-Time Hybrid Visualization Modality Combining Fluoroscopy and Segmented CT-Scan Facilitates Transcatheter Left Atrial Appendage Closure Procedure
By Igor V. Buzaev, Tagir Aminov, Vladimir Plechev, Irina Evgenievna Nikolaeva, Naufal Zagidullin, Eustaquio M. Onorato
Presenter
Igor V. Buzaev
Authors
Igor V. Buzaev1, Tagir Aminov2, Vladimir Plechev1, Irina Evgenievna Nikolaeva2, Naufal Zagidullin1, Eustaquio M. Onorato3
Affiliation
Bashkir State Medical University, Russian Federation1, Republican Cardiology Center, Russian Federation2, Monzino Cardiology Center, Italy3,
View Study Report
TCTAP C-165
STRUCTURAL HEART DISEASE - Left Atrial Appendage Closure
Real-Time Hybrid Visualization Modality Combining Fluoroscopy and Segmented CT-Scan Facilitates Transcatheter Left Atrial Appendage Closure Procedure
Igor V. Buzaev1, Tagir Aminov2, Vladimir Plechev1, Irina Evgenievna Nikolaeva2, Naufal Zagidullin1, Eustaquio M. Onorato3
Bashkir State Medical University, Russian Federation1, Republican Cardiology Center, Russian Federation2, Monzino Cardiology Center, Italy3,
Clinical Information
Patient initials or Identifier Number
NSM1953
Relevant Clinical History and Physical Exam
N. S. M., 68-year-old female was admitted to the Department of Interventional Cardiology on September 24, 2021 with complaints of irregular and faster heart beats during prolonged walking and shortness of breath (NYHA class II) since 2018. Atrial fibrillation was detected by ECG during outpatient clinic and the patient was treated with metoprolol, valsartan, and warfarin.
Relevant Test Results Prior to Catheterization
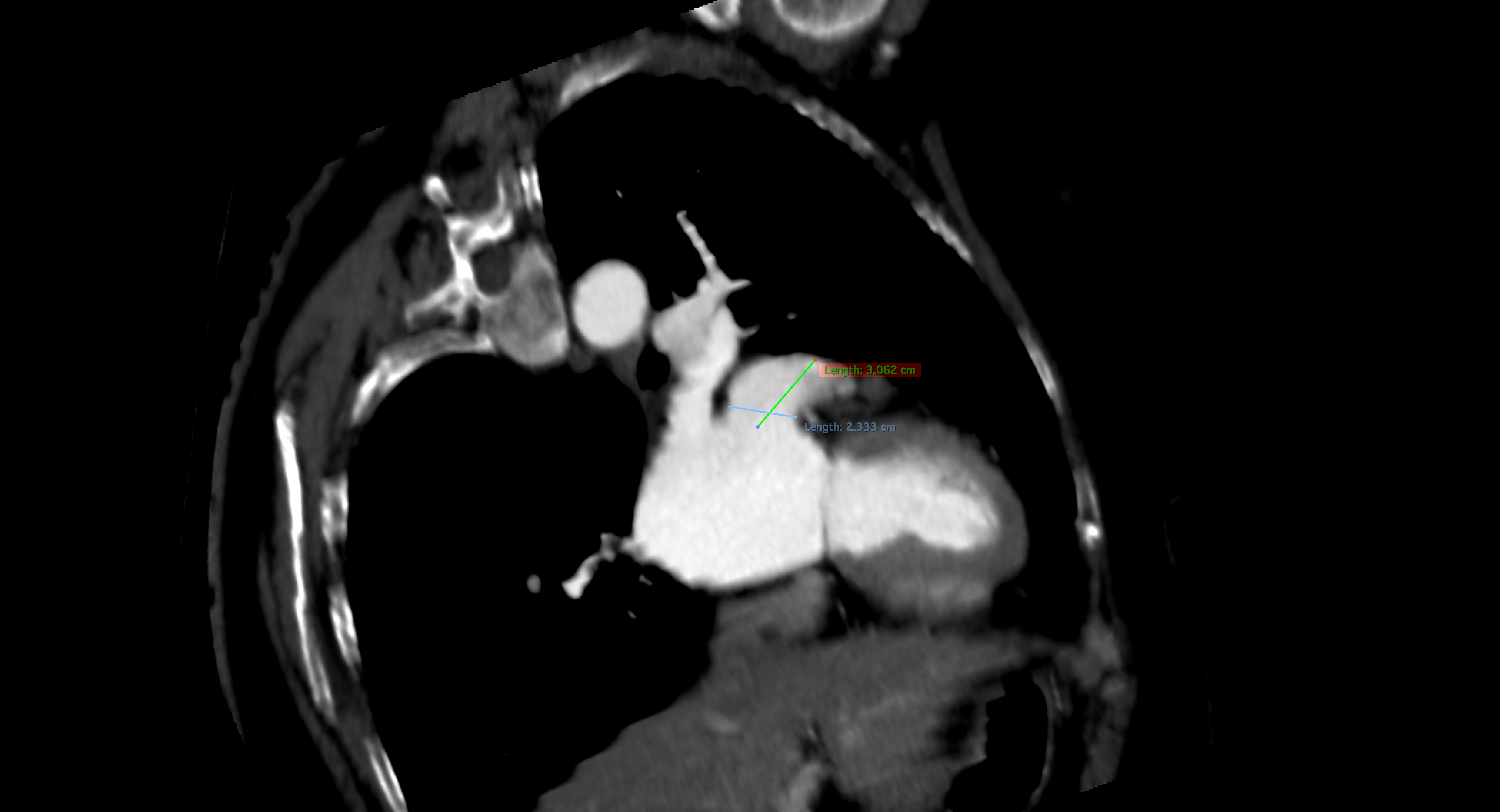
2D TEE color Doppler showed spontaneous contrasting in the left atrial cavity with a blood flow velocity in the left atrial appendage (LAA) of 50 cm/s without signs of blood clots. LAA dimensions were 1.9 cm x 3.4 cm. Chest CT angio (Figure 1) confirmed LAA volume up to 17 ml, 56 mm long, ostium appendage of 24 mm and the absence of inner thrombosis. CT angio scans have been segmentated using Phillips Heart Navigator software and uploaded to Philips angiographic system.
Relevant Catheterization Findings
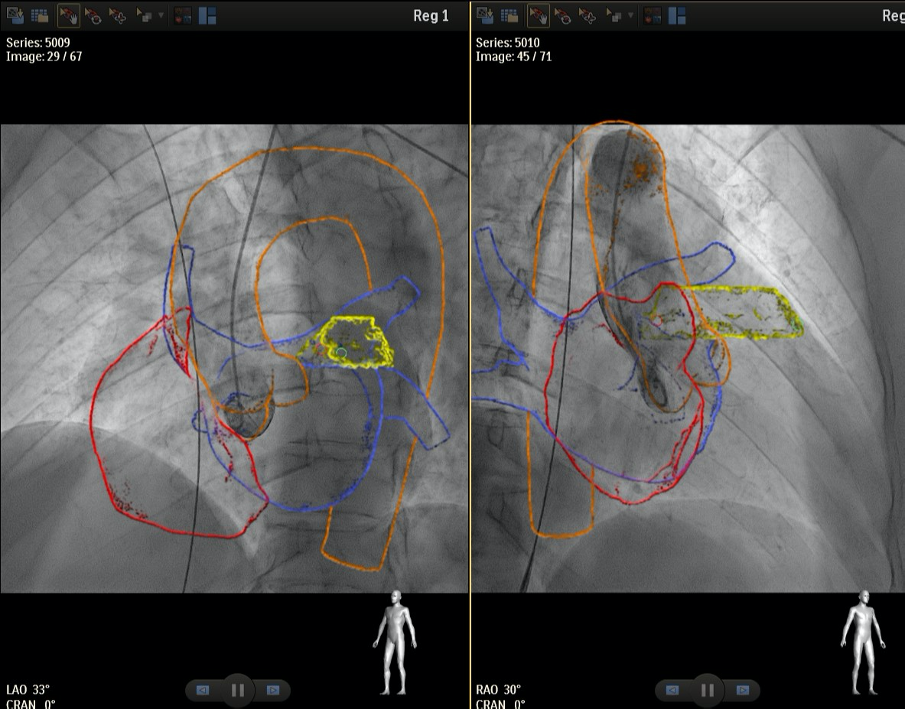
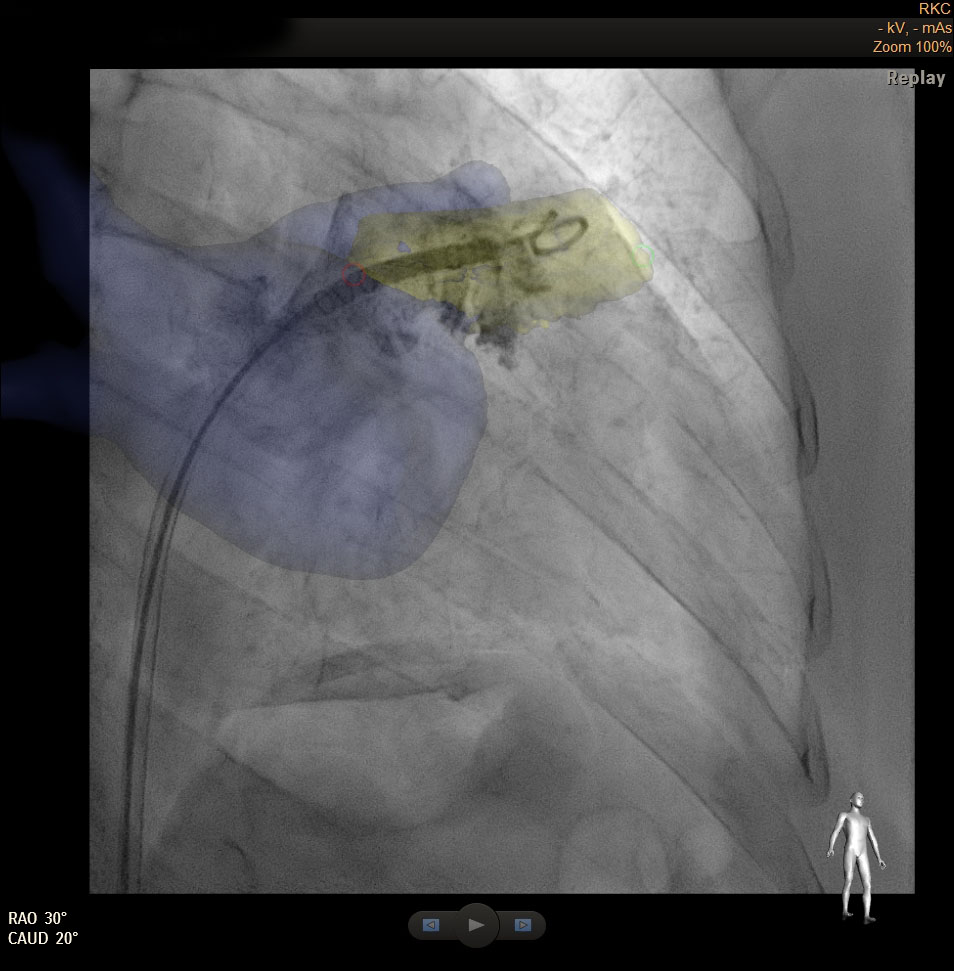
Right femoral venous and arterial approaches were used. Aortography was performed in two orthogonal projections to synchronize CT images on the fluoroscopic unit. The multispiral cardiac CT scan was synchronized with the angiographic picture using the HeartNavigator System (Fig. 2). After the transseptal puncture a 6-Fr pigtail catheter was placed in LAA for contrast injection. Fig. 3 showed the correspondence of angiographic picture and segmentated CT. LAA entrance size was measured as 24 mm.
Interventional Management
Procedural Step
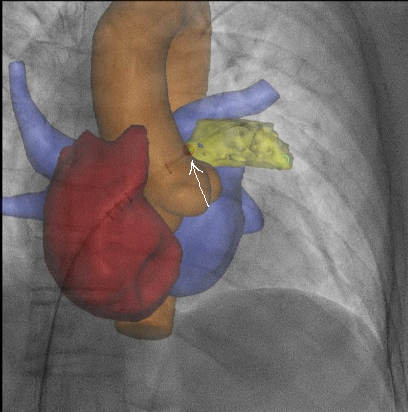
Transseptal puncture was done with the support of this hybrid visualization that resulted to be of paramount importance to understand x-ray negative structures of the heart (Fig. 4) in all C-arch positions (frontal, oblique, etc.).
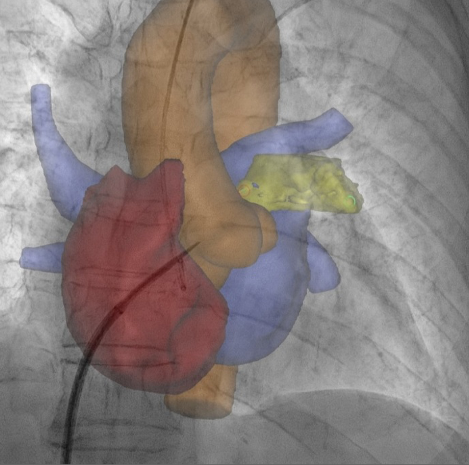
The dedicated delivery system 12F Angioline reached the left superior pulmonary vein and moved to LAA over the pigtail. Markers of the appendage ostium on segmented CT were set. These markers (Figure 5) were used as reference landmarks to deliver the LAA closure device 27 mm (Angioline). The presence of markers allowed us to position the occluder device safely and securely without the need for contrast injection and risk of embolism. After the opening of the device, a TEE check was performed (Figure 6). Contrast injection was done by hand. A pull-and-push maneuver was performed to check occluder stability and the device was successfully deployed. Patient was discharged home on the second postoperative day without any complication.
At 2-month follow up the patient remained symptom free and 2D transthoracic echocardiography confirmed stable position of the LAA occluder with no residual leaks.
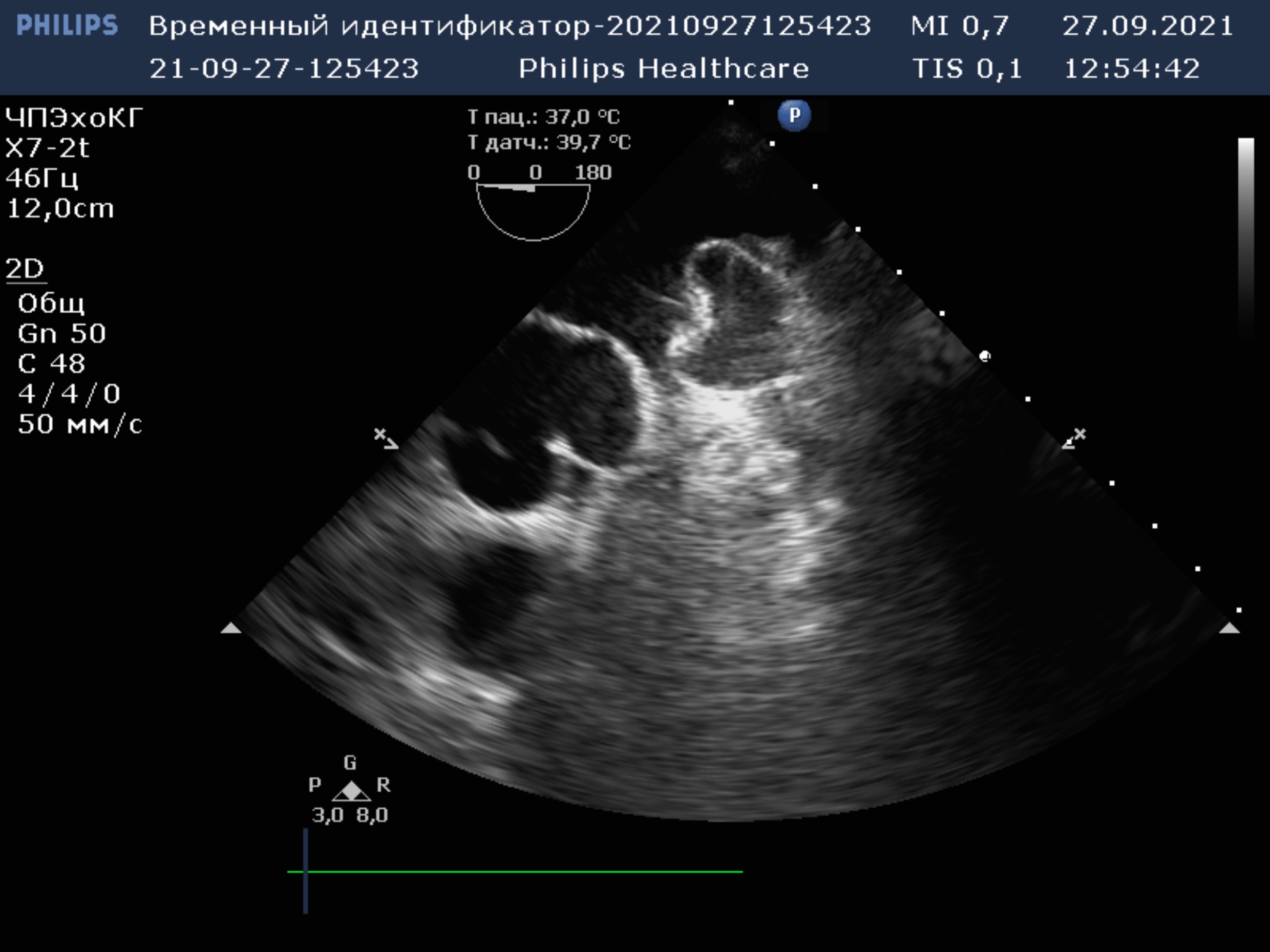
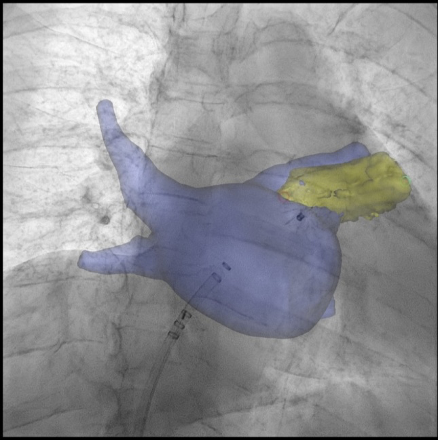
The dedicated delivery system 12F Angioline reached the left superior pulmonary vein and moved to LAA over the pigtail. Markers of the appendage ostium on segmented CT were set. These markers (Figure 5) were used as reference landmarks to deliver the LAA closure device 27 mm (Angioline). The presence of markers allowed us to position the occluder device safely and securely without the need for contrast injection and risk of embolism. After the opening of the device, a TEE check was performed (Figure 6). Contrast injection was done by hand. A pull-and-push maneuver was performed to check occluder stability and the device was successfully deployed. Patient was discharged home on the second postoperative day without any complication.
At 2-month follow up the patient remained symptom free and 2D transthoracic echocardiography confirmed stable position of the LAA occluder with no residual leaks.
Case Summary
1. The hybrid visualization modality by HeartNavigator System allows merging segmented CT-scan and real-time fluoroscopy. HeartNavigator System turned out to be useful to visualize x-ray negative structures and landmarks without contrast injection.
2. During LAA closure procedure, there are at least 2 crucial procedural steps where a good understanding of anatomical landmarks is necessary: transseptal puncture and implanting LAA occluder in the correct position.
3. HeartNavigator during LAA closure procedure may be key to successful definition of the relationships and landmarks of the anatomic structures.
2. During LAA closure procedure, there are at least 2 crucial procedural steps where a good understanding of anatomical landmarks is necessary: transseptal puncture and implanting LAA occluder in the correct position.
3. HeartNavigator during LAA closure procedure may be key to successful definition of the relationships and landmarks of the anatomic structures.