
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-059
Retrograde CTO RCA, Hard Stops !!
By Ramy Mohamed Atlm
Presenter
Ramy Mohamed Atlm
Authors
Ramy Mohamed Atlm1
Affiliation
Tanta University Hospital, Egypt1,
View Study Report
TCTAP C-059
CORONARY - Chronic Total Occlusion
Retrograde CTO RCA, Hard Stops !!
Ramy Mohamed Atlm1
Tanta University Hospital, Egypt1,
Clinical Information
Patient initials or Identifier Number
S A
Relevant Clinical History and Physical Exam
Male patient, aged 63 years old.
Known to be Diabetic, Not Hypertensive, with Cardiac history of Ischemic heart disease 2 months ago patient admitted with extensive anterior STEMI and undergo primary PCI to LAD with one DES, and his coronary angiography shows CTO RCA.
The patient Admitted to our center for elective PCI to CTO RCA.
Viability study was done and shows ischemic viable apico and mid inferior, infero-lateral, infero-septal walls
So,,, We decided to go for PCI to CTO RCA.
Known to be Diabetic, Not Hypertensive, with Cardiac history of Ischemic heart disease 2 months ago patient admitted with extensive anterior STEMI and undergo primary PCI to LAD with one DES, and his coronary angiography shows CTO RCA.
The patient Admitted to our center for elective PCI to CTO RCA.
Viability study was done and shows ischemic viable apico and mid inferior, infero-lateral, infero-septal walls
So,,, We decided to go for PCI to CTO RCA.
Relevant Test Results Prior to Catheterization
ECG: Normal sinus rhythm with Qs STelevation in anterior leads ( old anterior STEMI ) and T wave inversion in inferior leads.
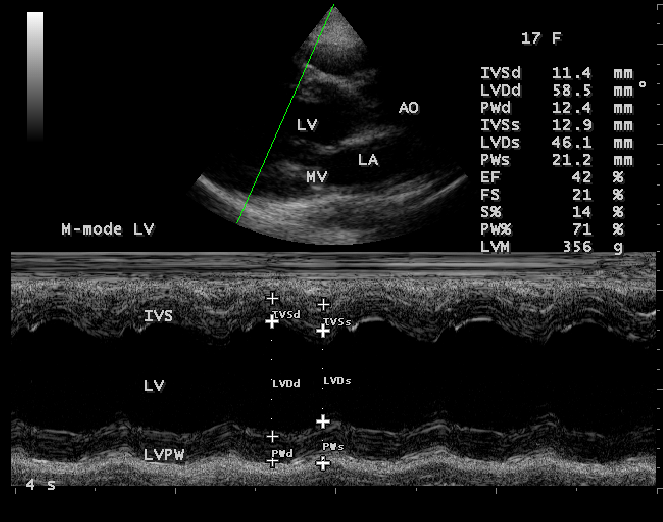
ECHO: Ischemic heart disease with average systolic function, RSWMAs in the form of ( Apico-anterior, mid and basal anterior and anteroseptal, inferior and infero-septal wall hypokinesia ), with moderate mitral valve incompetence
All laboratory investigations were unremarkable.

ECHO: Ischemic heart disease with average systolic function, RSWMAs in the form of ( Apico-anterior, mid and basal anterior and anteroseptal, inferior and infero-septal wall hypokinesia ), with moderate mitral valve incompetence
All laboratory investigations were unremarkable.
Relevant Catheterization Findings
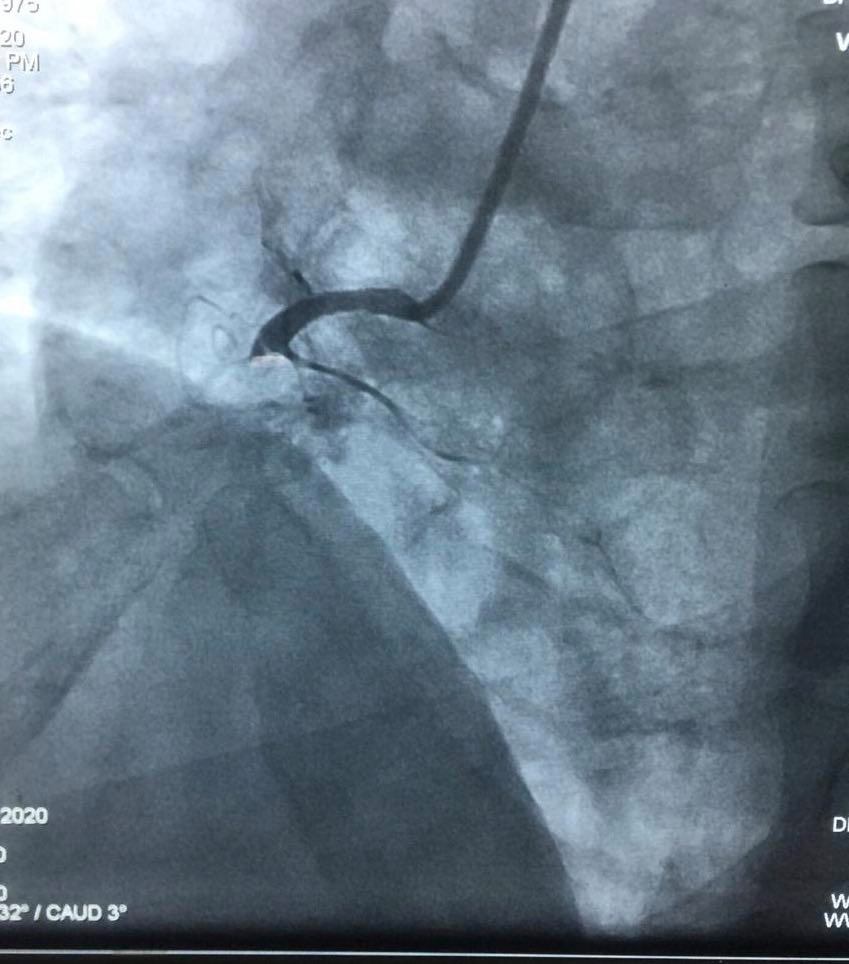
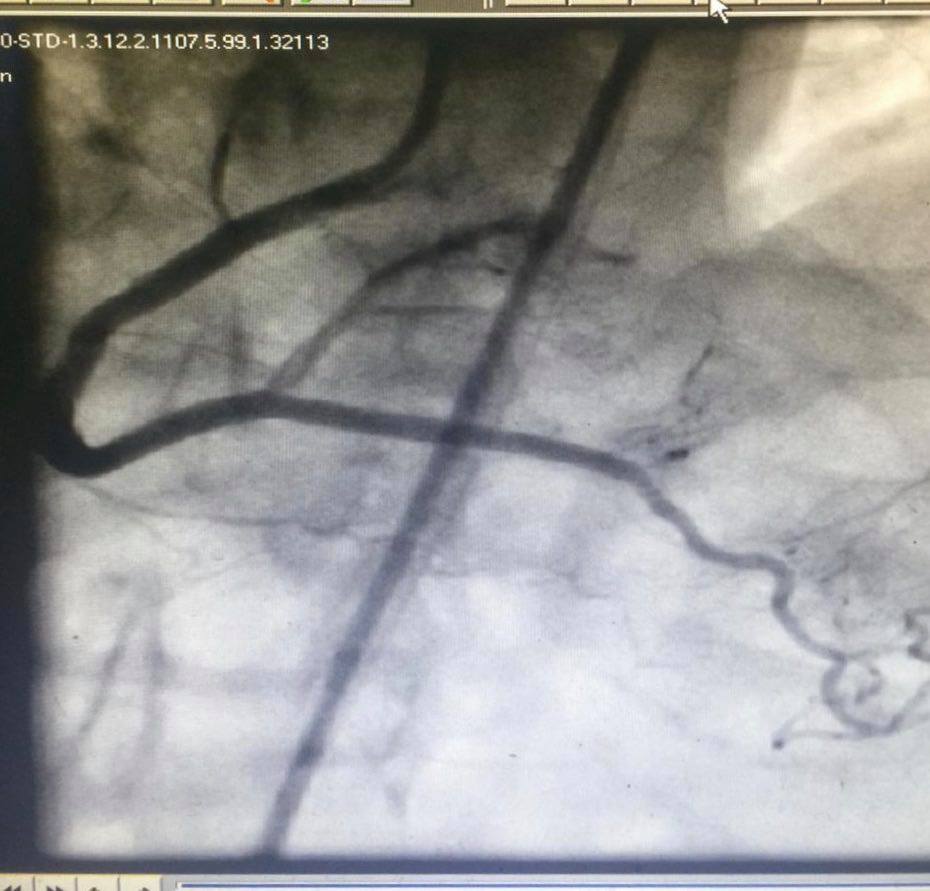
LM : Normal bifurcating into LAD and LCX LAD : Atherosclerotic vessel with patent previously pre-deployed stent LCX : Atherosclerotic vessel with non significant lesionRCA : Atherosclerotic vessel with proximal total occlusion receiving retrograde collaterals from septal branches of LAD
 Retrograde CTO RCA Hard stops.pptx
Retrograde CTO RCA Hard stops.pptx
Interventional Management
Procedural Step
- Wiring of RCAante-gradely by BMW wire with advancement of Caravel MC
Failed Antegrade trial (AWE) by Fielder XTA followed by GAIA 2nd on caravel MC
- Antegrade and Retrograde Injection was done through JR 4 and XB 4 6F Guiding catheters
- Wiring of LADby BMW wire with advancement of Caravel MC
Exchanging BMWwire through microcatheter by Sion blue wire
- Then Septalsurfing by Sion blue wire
The advancement of Sion blue wire through septal collaterals followed by MC advancement till distal cap
Sion blue wire was exchanged through microcatheter by GAIA 2nd wire with piercing of distal cap by GAIA 2ndGAIAfailed to go through CTO Body
Followed by negotiation of CTO body by Pilot200 and Fielder XTA
So, We decidedto go via Reversed CART technique Antegrade: pilot 200 and balloon together with anchor wire in conus branch
Retrograde: GAIA 2nd and Caravel MC
Successful passage of conquest pro 12 through retrograde subintimal space to antegrade subintimal space to true lumen
So, Snaringfrom aorta
Advancement of Caravel microcatheter again into retrograde Guiding through collateral but microcatheter failed to cross CTO segment
So, balloon trapping of retrograde wire by antegrade balloon
With successful passage of MC into antegrade guide followed by replacement of conquest pro 12by RG3 wire
Withdrawal ofCaravel microcatheter Then dilatation and stenting
Failed Antegrade trial (AWE) by Fielder XTA followed by GAIA 2nd on caravel MC
- Antegrade and Retrograde Injection was done through JR 4 and XB 4 6F Guiding catheters
- Wiring of LADby BMW wire with advancement of Caravel MC
Exchanging BMWwire through microcatheter by Sion blue wire
- Then Septalsurfing by Sion blue wire
The advancement of Sion blue wire through septal collaterals followed by MC advancement till distal cap
Sion blue wire was exchanged through microcatheter by GAIA 2nd wire with piercing of distal cap by GAIA 2ndGAIAfailed to go through CTO Body
Followed by negotiation of CTO body by Pilot200 and Fielder XTA
So, We decidedto go via Reversed CART technique Antegrade: pilot 200 and balloon together with anchor wire in conus branch
Retrograde: GAIA 2nd and Caravel MC
Successful passage of conquest pro 12 through retrograde subintimal space to antegrade subintimal space to true lumen
So, Snaringfrom aorta
Advancement of Caravel microcatheter again into retrograde Guiding through collateral but microcatheter failed to cross CTO segment
So, balloon trapping of retrograde wire by antegrade balloon
With successful passage of MC into antegrade guide followed by replacement of conquest pro 12by RG3 wire
Withdrawal ofCaravel microcatheter Then dilatation and stenting
Case Summary
1- The antegrade route should generally be considered as the primary approach; however, prior to all CTO procedures, it is essential to assess the eligibility of the patient and the lesion for a retrograde approach in order to be prepared to change the strategy.