
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-085
Primary V-A ECMO-Supported Retrograde CTO PCI via the Large, Last-Remaining and Indispensable Collateral
By Wei-Jhong Chen
Presenter
Wei-Jhong Chen
Authors
Wei-Jhong Chen1
Affiliation
Taichung Veterans General Hospital, Taiwan1,
View Study Report
TCTAP C-085
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Primary V-A ECMO-Supported Retrograde CTO PCI via the Large, Last-Remaining and Indispensable Collateral
Wei-Jhong Chen1
Taichung Veterans General Hospital, Taiwan1,
Clinical Information
Patient initials or Identifier Number
Yang
Relevant Clinical History and Physical Exam
Sex:male
Age:66years old
Past history: Hypertension,for more than 10 years
Chief complaint:
Abruptonset of chest piercing pain with cold sweating in 2020/06
CAD, TVD, found at other hospital; CABGsuggested
Relevant Test Results Prior to Catheterization
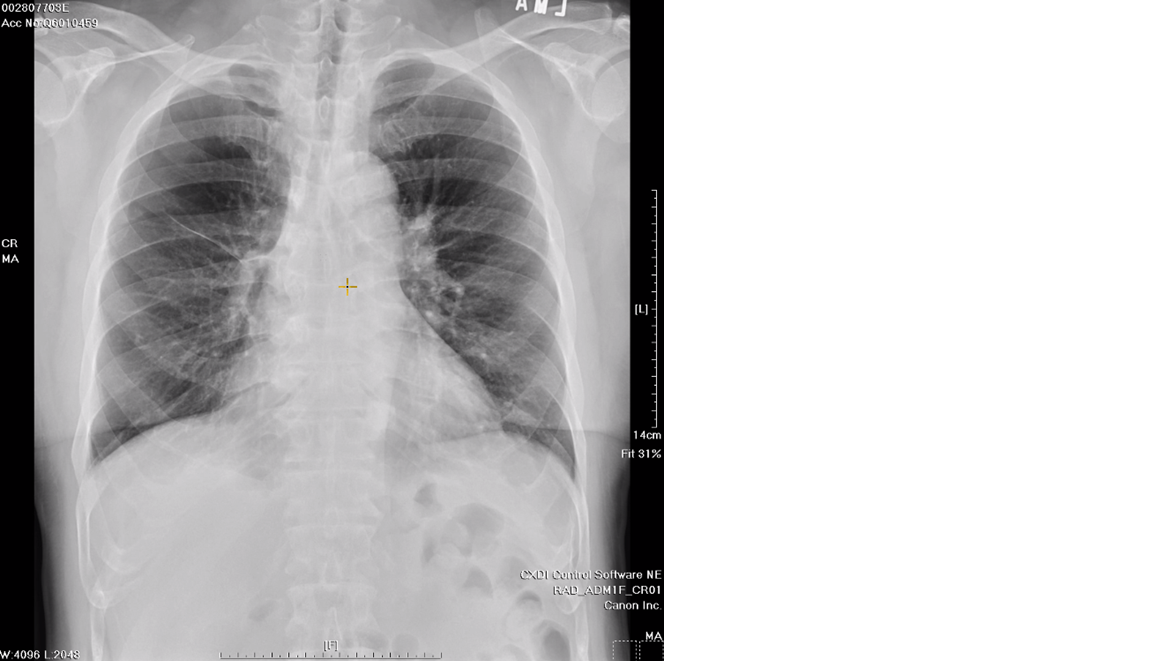
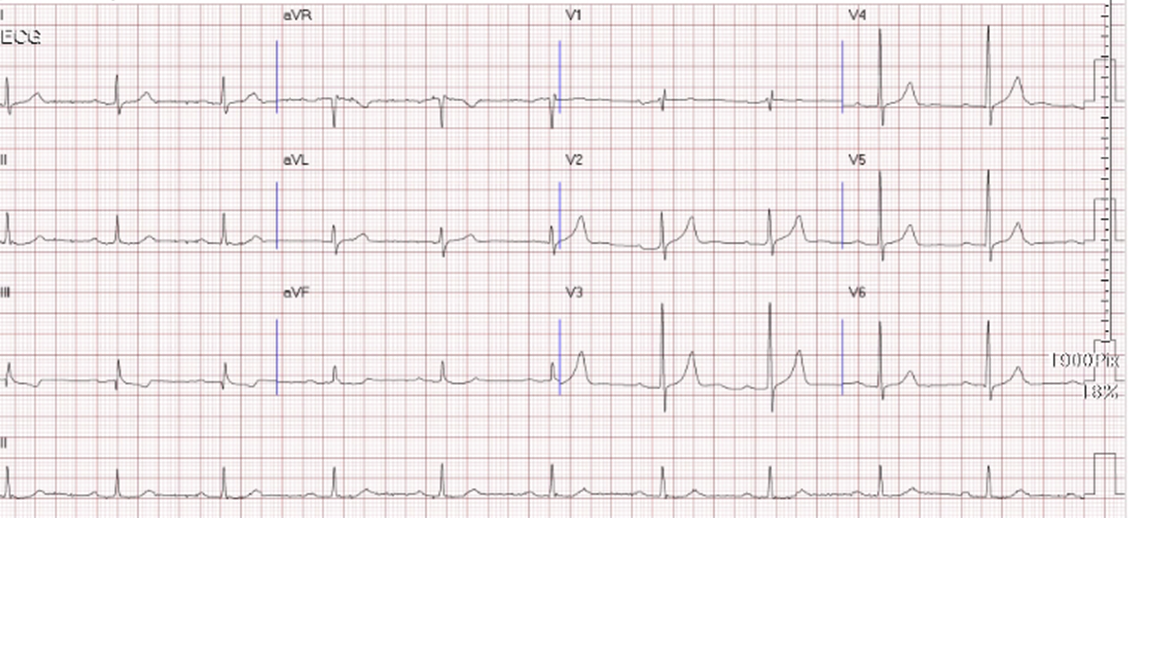
Hemoglobin: 13.4 gm/dlPlatelet: 166X 103/uLCrea: 1.14 mg/dlALT: 46 U/LPT(INR): 10.4(1.0)aPTT: 26.4 secCXR and ECG as uploaded image
Relevant Catheterization Findings
CAG finding:Bil. CAG : right dominant.LAD: severe AS changes
 Diagnostic angiogram-RCA.wmv
Diagnostic angiogram-RCA.wmv
Diagnostic angiography-LCA-1.wmv
Diagnostic angiography-LCA-2.wmv
Interventional Management
Procedural Step
PCI on 2020/07/08
ECMO deploy.wmv
Third PCI-1.wmv
Third PCI-2.wmv
Case Summary
Patience and trust on both physicianand patient sides play important role in forging revascularization strategy.
Treatment planning tailored to asingle patient is an important key to successful CTO PCI.
Occluding a large last-remining andindispensable collaterals could result in severe hemodynamic compromise and chest pain during retrograde PCI and precludes further attempt.
ECMO, particularly primary, is an integral part of CHIP intervention and provides good temporary hemodynamic support, allowing retrograde PCI to continue in these cases.