
Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-166
Percutaneous Pulmonic Balloon Valvuloplasty in Carcinoid Heart Disease With Bioprosthetic Tricuspid Valve
By Bryan Rene Toledano, Kristy Garganera, Jessielyn Sia, Luis Martin Icasiano Habana, Timothy Dy
Presenter
Bryan Rene Toledano
Authors
Bryan Rene Toledano1, Kristy Garganera1, Jessielyn Sia2, Luis Martin Icasiano Habana1, Timothy Dy2
Affiliation
The Medical City, Philippines1, Chinese General Hospital and Medical Center, Philippines2,
View Study Report
TCTAP C-166
STRUCTURAL HEART DISEASE - Others (Structural Heart Disease)
Percutaneous Pulmonic Balloon Valvuloplasty in Carcinoid Heart Disease With Bioprosthetic Tricuspid Valve
Bryan Rene Toledano1, Kristy Garganera1, Jessielyn Sia2, Luis Martin Icasiano Habana1, Timothy Dy2
The Medical City, Philippines1, Chinese General Hospital and Medical Center, Philippines2,
Clinical Information
Patient initials or Identifier Number
GM
Relevant Clinical History and Physical Exam
A 52 year old female presented with easy fatiguability. She is a known case of Carcinoid tumor stage IV with multiple hepatic metastases. She underwent ileal resection, Transarterial chemoembolization, Selective Internal Radiation and Tricuspid bioprosthetic valve replacement for severe TR last 2018. She is on monthly ocreotide injections. On physical examination a mid systolic crescendo-decresendo murmur heard best at 2nd left ICS right sternal border accentuated during inspiration was noted.
Relevant Test Results Prior to Catheterization
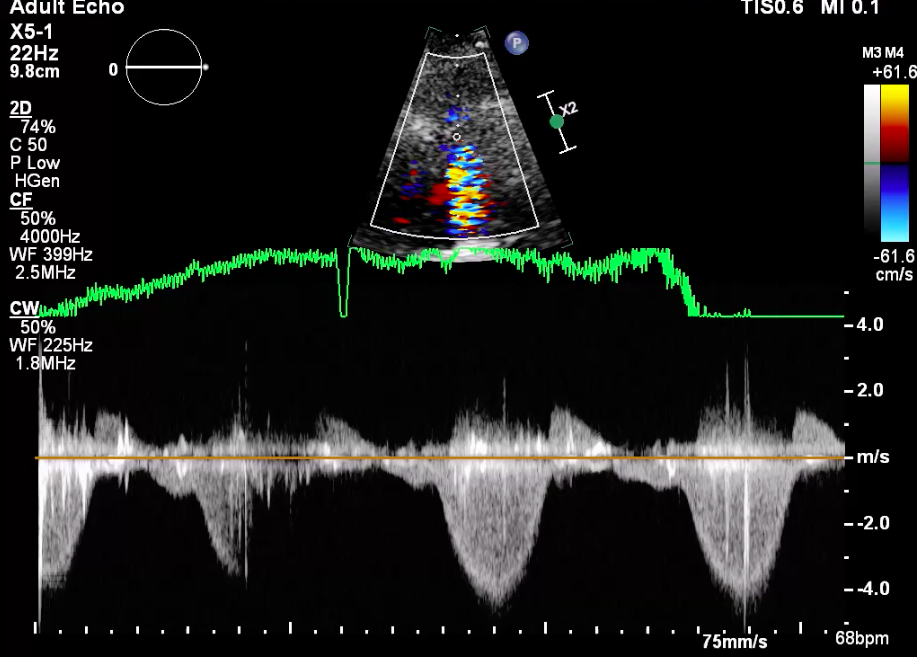
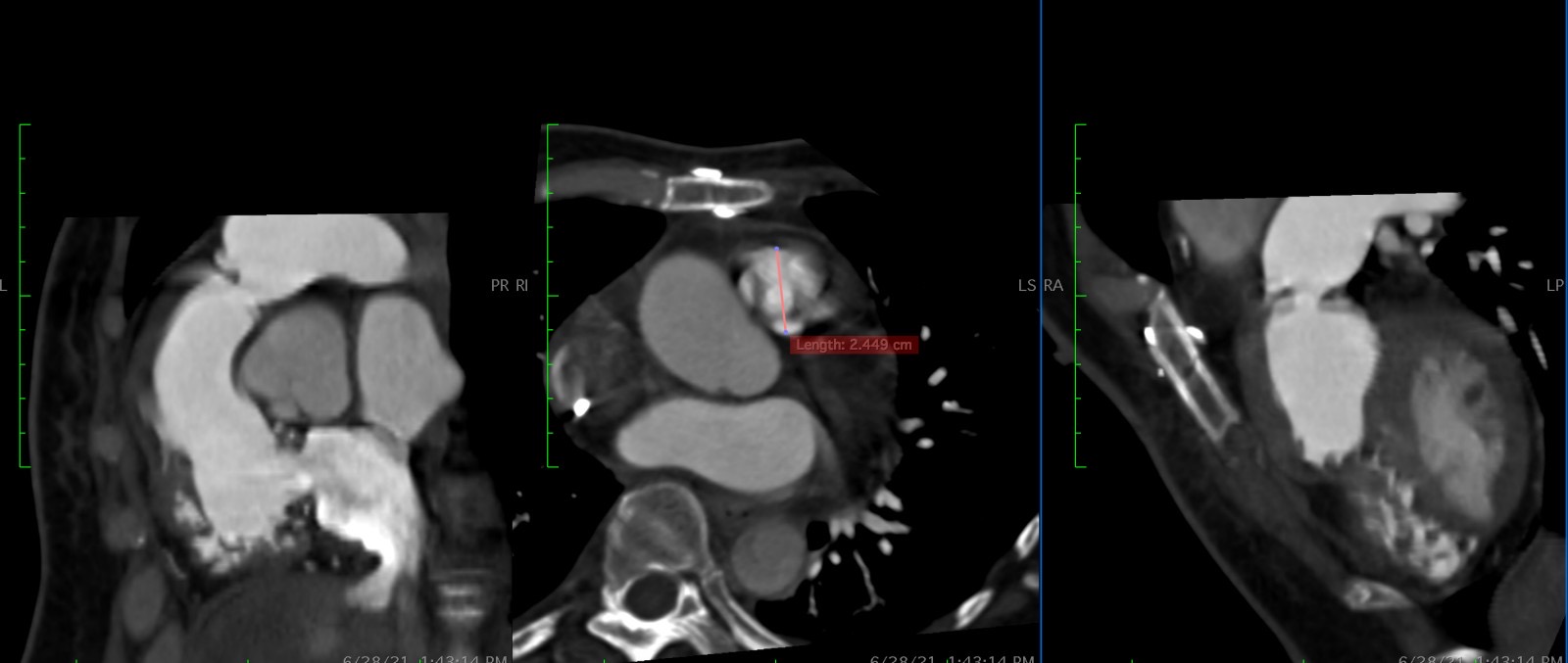
Her urine 5-HIAA was elevated at 125.9mg/24. On 2D echocardiogram the bioprosthetic TV was structurally normal but the right atrium was dilated and the right ventricle hypertrophied. A severe pulmonic stenosis, peak gradient of 85mmhg and mild pulmonic regurgitation was seen. The RVFAC was normal at 43% however on post-process analysis using speckle tracking a decreased RV lateral shortening of 12.9% was noted. A cardiac CT scan measured a PV planimetry of 0.29cm2 and an annulus of 24mm.
 Pulmoic Valve.mov
Pulmoic Valve.mov
Relevant Catheterization Findings
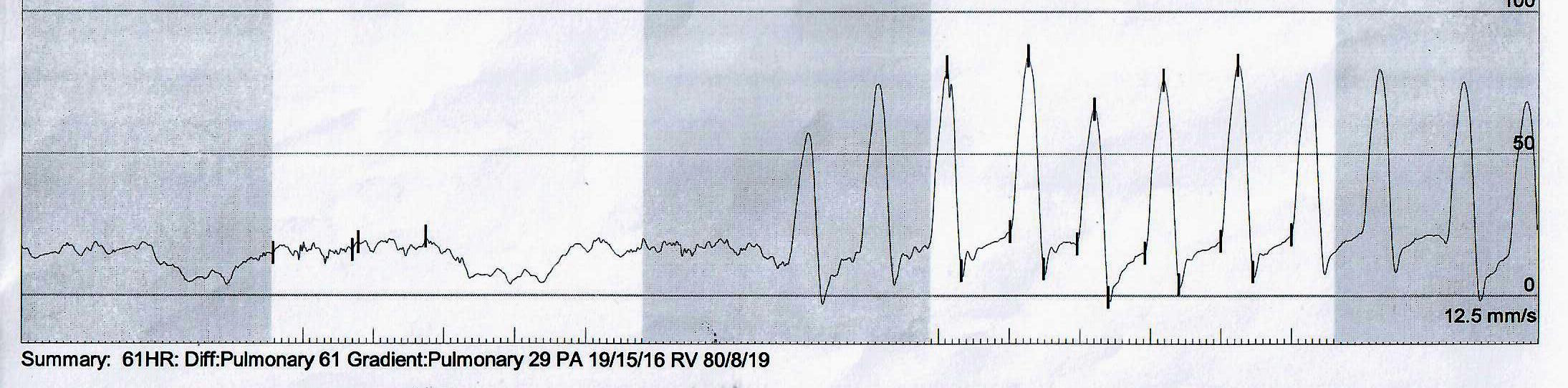
On right ventriculogram the ventricle was hypertrophied with preserved systolic function. The pulmonary valve was thickened with a jet of contrast in a small orifice-dooming valve. A poststenotic dilatation of the main pulmonary and left and right pulmonary arteries were also seen. A pull back gradient of 61mmhg was obtained from a pulmonary artery pressure of 19/15 (16)mmhg and a right ventricular pressure of 80/8mmhg.
AP view pre PPBV.mov
Lateral view pre PPBV RV gram.mov
Interventional Management
Procedural Step
In the cardiac catheterisation laboratory under intravenous sedation and sterile conditions the right femoral vein was accessed using an 8F sheath via Seldinger technique. A pigtail catheter with the straight end of the J wire was used for antegrade advancement to the right atrium, prosthetic tricuspid valve and right ventricle. A Terumo glide wire supported by 7F JR 5 Mach catheter was used to cross the stenotic pulmonic valve. An Amplatz stiff wire was introduced as an exchange and was advanced deep into the left pulmonary artery (PA). Before ballooning using an 8F JR 4 guide catheter a pullback gradient of 61mmHg was obtained. The PA pressure was 19/15 (16)mmHg and the right ventricular pressure was 80/8mmHg. The femoral sheath was exchanged to Sentrant 14F to accommodate the Z-Med II percutaneous transluminal valvuloplasty (PTV) catheter size 23mm x 4 cm which was positioned and inflated in the pulmonic valve and right ventricular outflow tract for 3 seconds. Again using an 8F JR 4 guide catheter a repeat pullback gradient, decreased to 24mmHg from a baseline of 61mmHg. The PA pressure was 24/16 (14)mmHg and RV pressure was 48/18 mmHg. Hence a second inflation using a larger PTV catheter sized 26mm x 4cm was done. After this a pullback gradient of 3 mmHg with a PA pressure of 24/16 (14)mmhg and RV pressure of 27/16 mmHg was achieved. A repeat right ventriculogram revealed a markedly improved mobility of the valve leaflets with larger valve orifice.
AP view 2nd PPBV.mov
Lateral view post PPBV RV gram.mov

Case Summary
Carcinoid Heart with Hepatic Metastases is rare disease that variably affects the tricuspid and pulmonic valves. A cardiac computed tomography scan is an invaluable tool to measure the pulmonic valve annulus for proper balloon sizing. Percutaneous Pulmonic Balloon Valvuloplasty carries a lower risk for crisis, immediately improves echocardiographic parameters of the right ventricle in preparation for hepatic cytoreductive surgery. In the presence of a bioprosthetic tricuspid valve, careful advancement of wires and catheters is important to avoid entanglement. Finally a gradual step-up of balloon size should be done to avoid rupture and to achieve the desired gradient for symptom relief.