Lots of interesting abstracts and cases were submitted for TCTAP 2022. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP A-021
The Major Difference Between Diamondback and Rotablator ~Aspect From Bench Test~
By Takuma Tsuda, Nao Yasuda
Presenter
Takuma Tsuda
Authors
Takuma Tsuda1, Nao Yasuda1
Affiliation
Nagoya Ekisaikai Hospital, Japan1
View Study Report
TCTAP A-021
Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
The Major Difference Between Diamondback and Rotablator ~Aspect From Bench Test~
Takuma Tsuda1, Nao Yasuda1
Nagoya Ekisaikai Hospital, Japan1
Background
Orbital atherectomy system (OAS) has been more common device for calcified lesion in Japan. However, the effect of OAS in bending artery have been remained unclear. The aim of this study is to make clear how OAS do work by bench test.
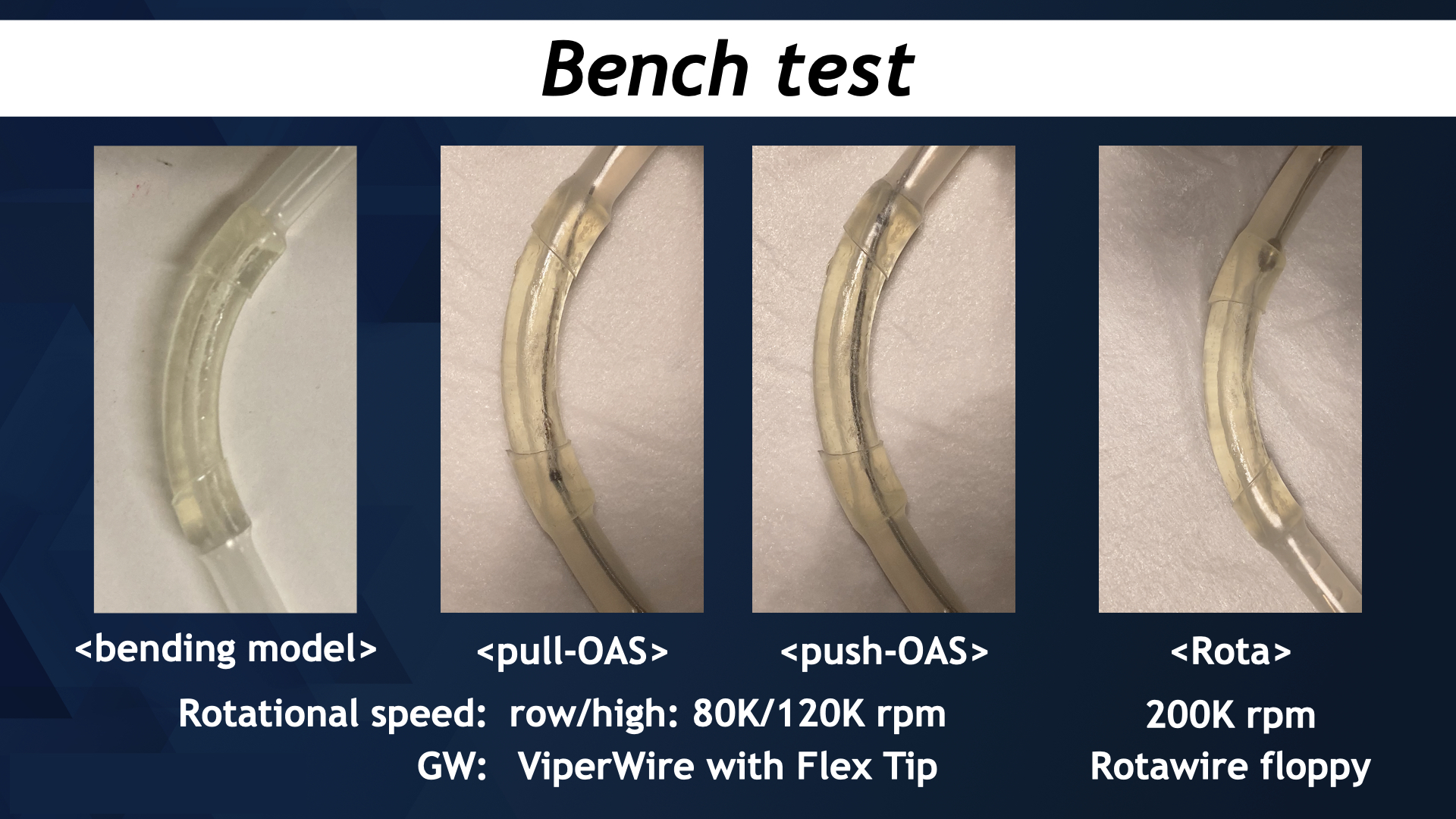
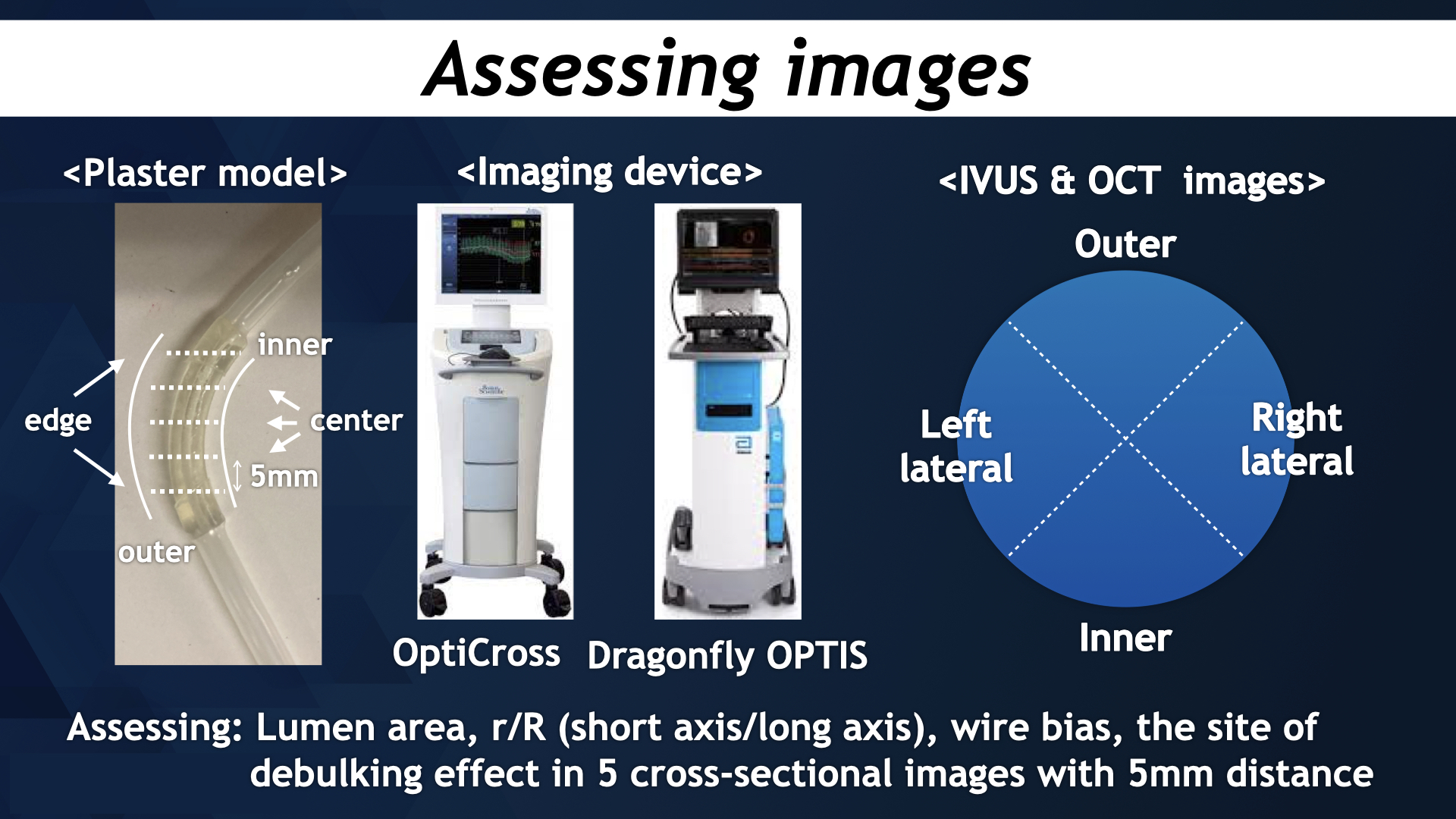
Methods
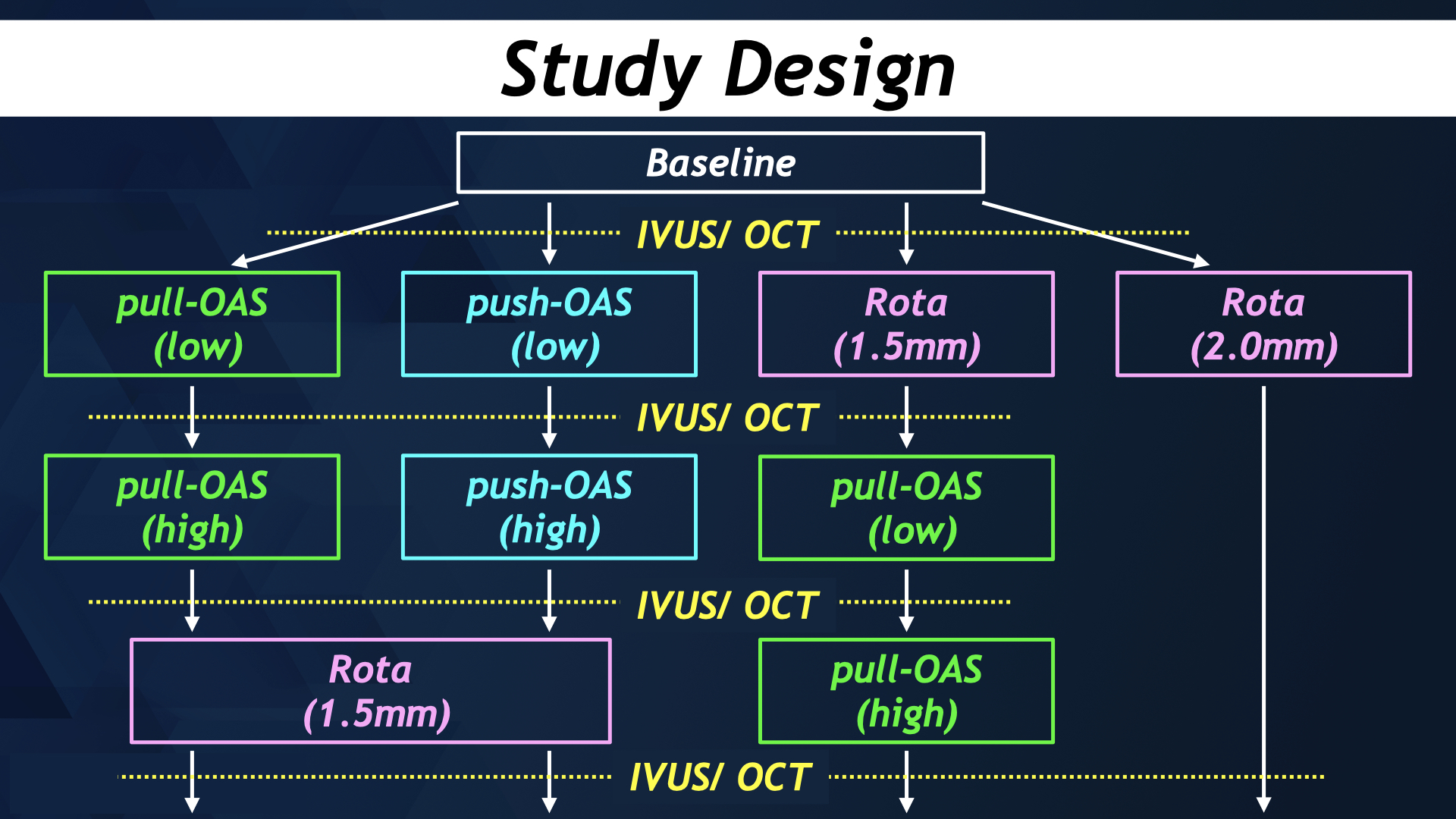
We performed bench test by bending plaster model. Rotablator (ROTA PRO; Boston Scientific, Japan) was performed with Rotafloppy (Boston scientific, Japan), by 200 Krpm. OAS (Diamondback; Medikit, Japan) was performed with both pullback and push manner with ViperWire with FlexTip (Medikit, Japan) by both low-speed (80 Krpm) or high-speed (120 Krpm). Each procedure was assessed by imaging modality with both IVUS (OptiCross HD; Boston scientific, Japan) and OCT (Dragonfly OpStar; Abbott, Japan). We assessed push-OAS, pull-OAS and rotablator by assessing cross-sectional images of IVUS or OCT with each 5 mm length. Moreover, and compared the site of debulking effect and device bias in each cross-sectional images.
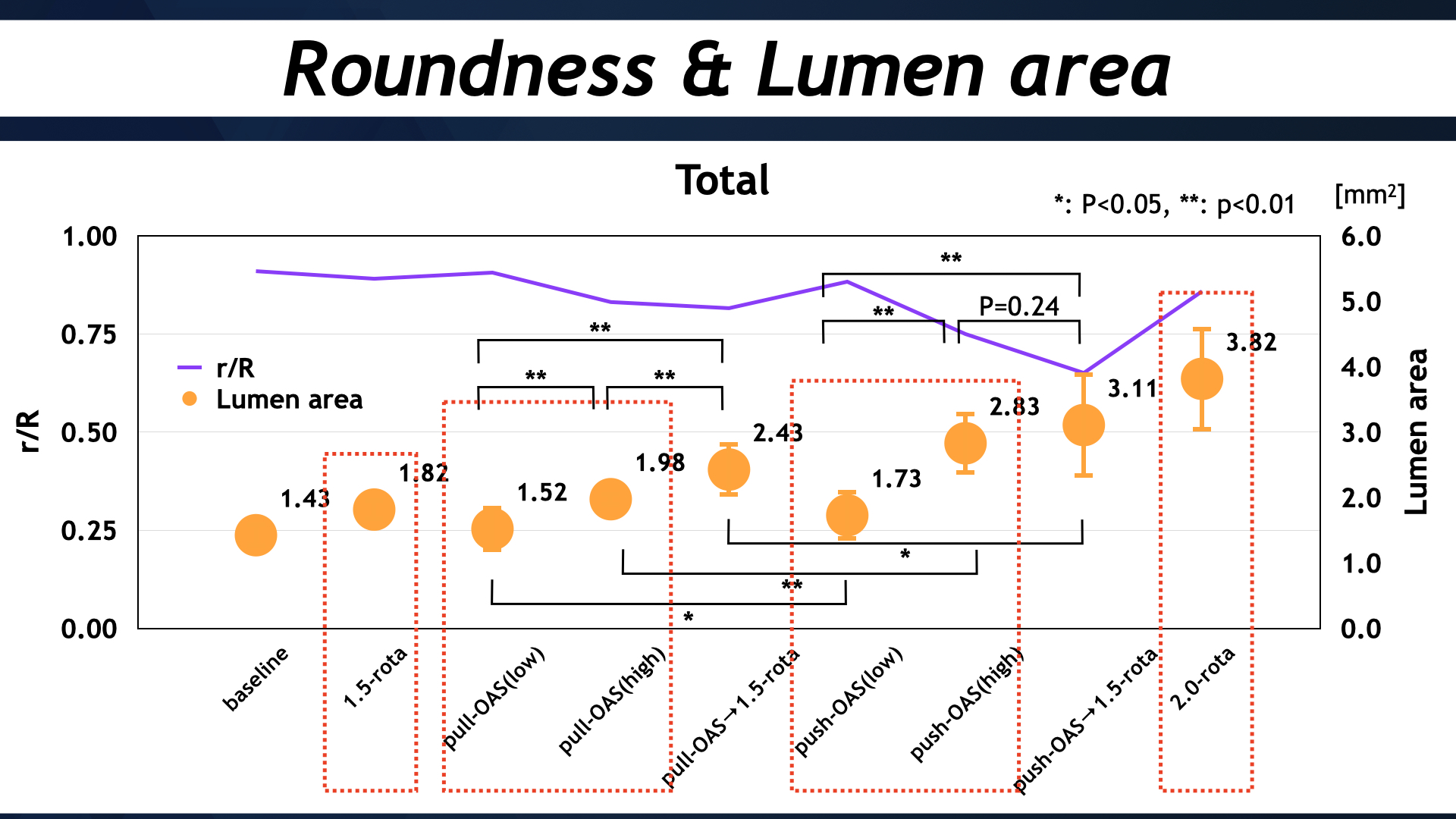
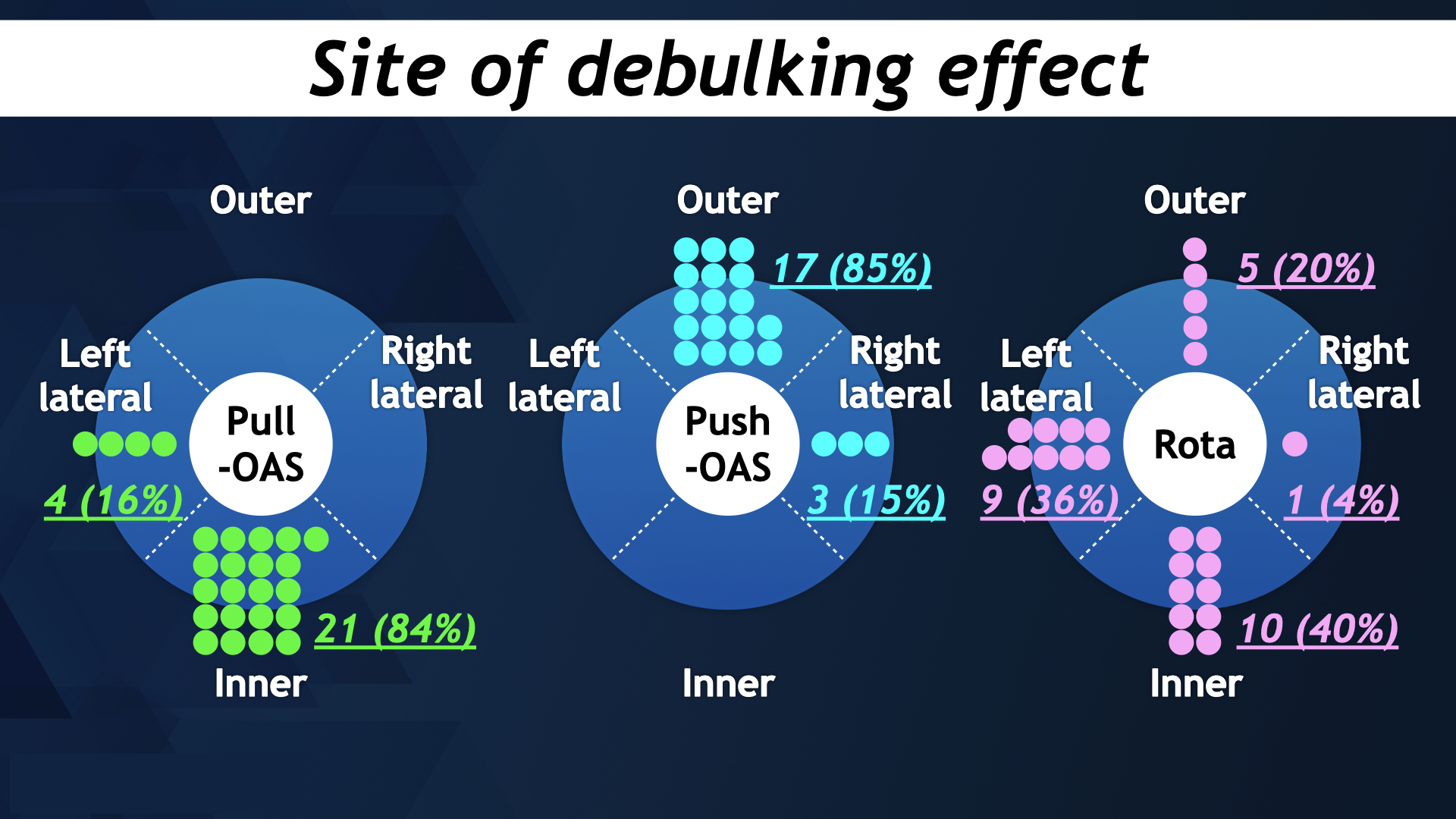
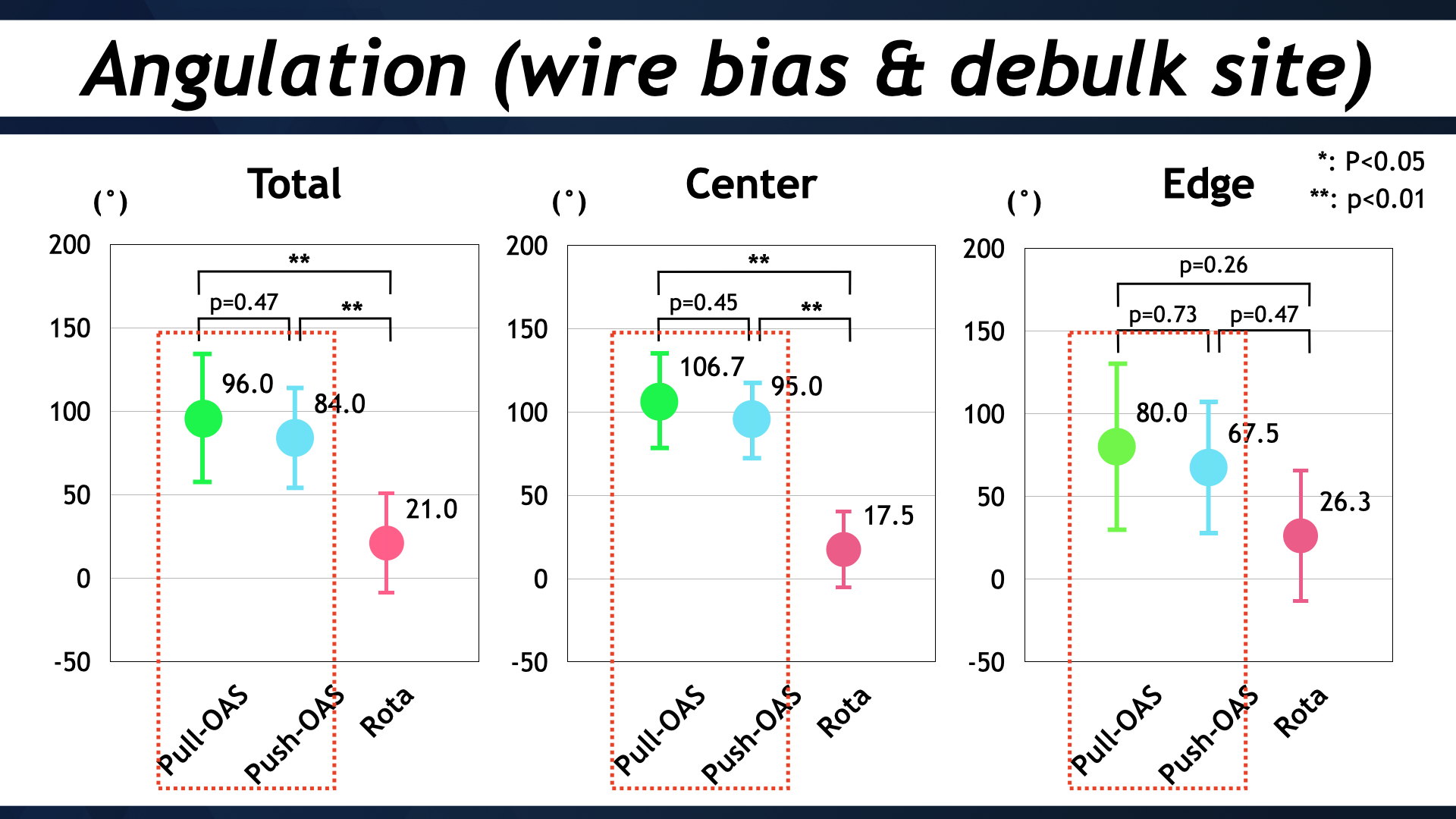
Results
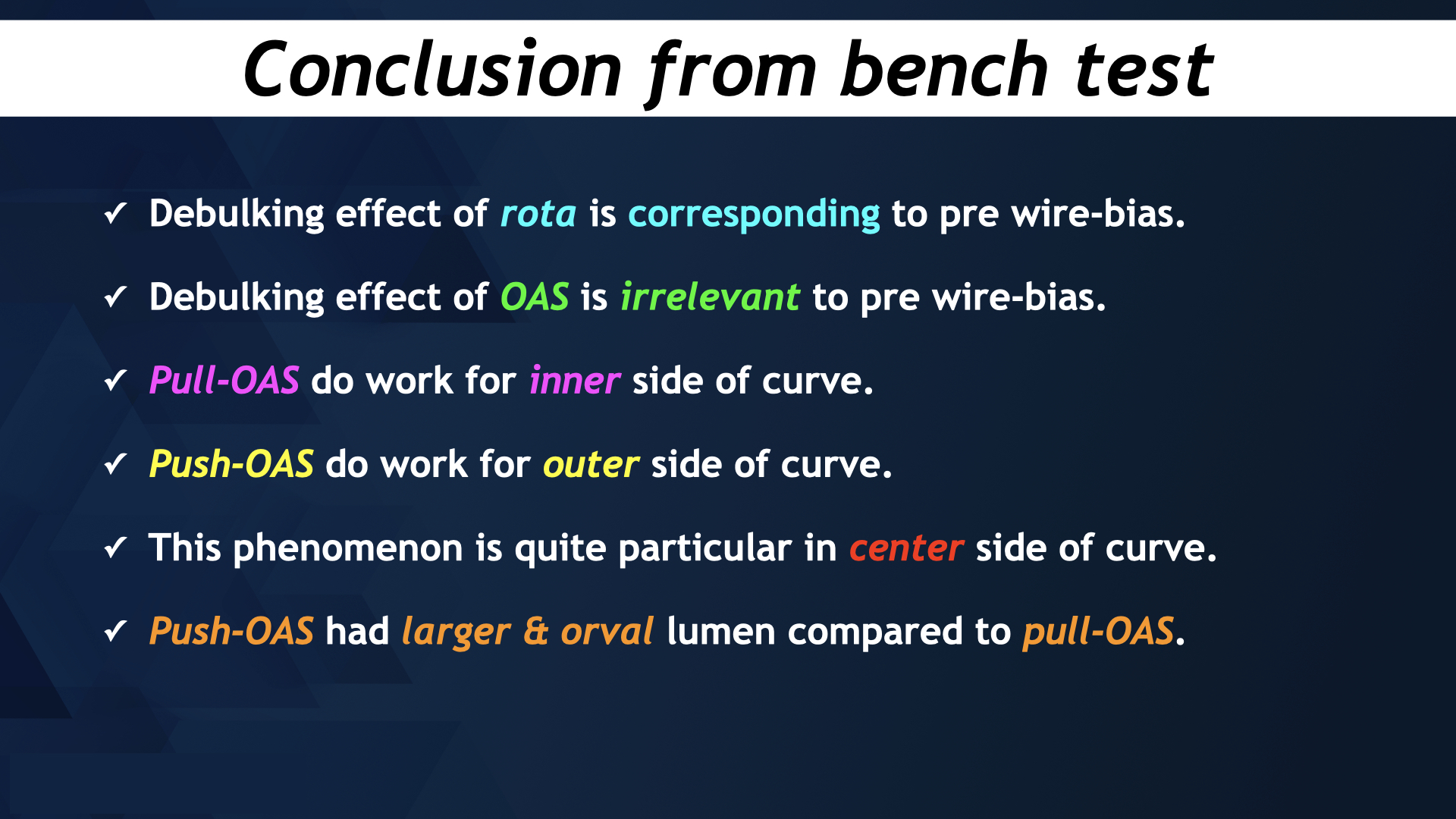
Push-OAS (2.83 ± 0.39 mm2) have larger lumen compared pull-OAS (1.98 ± 0.35 mm2) or 1.5mm rotablator (1.82 ± 0.20 mm2), however, it was smaller than 2.0mm rotablator (3.82 ± 0.80 mm2) (p < 0.05). Moreover, Push-OAS have more orval shape than pull-OAS or rotablator (r/R = 0.75 ± 0.06 vs 0.83 ± 0.05 vs 0.88 ± 0.08, p < 0.05). Correlation between debulking effects and bias in both pull-OAS and push-OAS were less compared with those in rotablator (21 ± 31° vs 96 ± 51° vs 84 ± 39°, p < 0.01). Moreover, debulking effect of pull-OAS localized at inner side of curve (84%), since those of push-OAS did at outer side of curve(85%).
Conclusion
OAS have quite different from rotablator concerned about debulking site, and this outcome could contribute for understanding the way of motion of OAS and reduction of procedural complication in bending artery.