

 Gregg W. Stone, MD (Icahn School of Medicine at Mount Sinai, New York, USA) and Seung-Jung Park, MD (Asan Medical Center, Seoul, South Korea) discussed treatment strategies for vulnerable plaques on April 22 during the “Main Area” lecture at TCTAP 2021 Virtual.
Gregg W. Stone, MD (Icahn School of Medicine at Mount Sinai, New York, USA) and Seung-Jung Park, MD (Asan Medical Center, Seoul, South Korea) discussed treatment strategies for vulnerable plaques on April 22 during the “Main Area” lecture at TCTAP 2021 Virtual.
Since the release of the original PROSPECT study 10 years ago, interest in treatment of vulnerable plaques has grown.
During the session, Stone highlighted results from accumulated clinical evidence on vulnerable plaques and Park continued with an update on the current status of the PREVENT trial.
“There are now several credible methods for evaluating vulnerable plaque that include coronary CT angiography, IVUS, VH-IVUS, NIRS, and OCT,” Stone said. “All these can identify vulnerable plaque with their own specific characteristics such as positive remodeling, plaque burden, lipid rich plaque and thin-cap fibroatheromas.”
The original PROSPECT study evaluated the non-culprit lesion plaque characteristics among 700 acute coronary syndrome (ACS) patients.
Various vulnerable plaque features (plaque burden ≥70%, minimal luminal area ≤4.0mm2 and VH-IVUS defined thin-cap fibroatheroma (TCFA), etc.) were equally attributable to major adverse cardiovascular events (MACE) when found in either non-culprit or culprit lesions.
This led to the conclusion that plaque imaging may play an important role in identifying at-risk lesions, especially for unexpected adverse cardiac events associated with non-culprit lesions.
In contrast to the PROSPECT study, the Lipid Risk Plaque Study published in the Lancet in 2019 included 1,500 stable angina patients in half of the population, and showed the segment with a maxLCBI4mm ≥400 by NIRS had an unadjusted hazard ratio (HR) of 4.2 for non-culprit lesion (NCL)-MACE at two years.
The subsequent PROSPECT II and COMBINE OCT-FFR trial results presented at TCT 2020. PROSPECT II enrolled 900 ACS patients and showed that NIRS-defined lipid rich plaque and IVUS-defined plaque burden were found to be the most powerful determinants for four years of NCL-MACE. Those findings established the lipid rich plaque on NIRS as a feature of vulnerable plaque.
The COMBINE OCT-FFR trial enrolled more than 500 diabetic patients with stable ACS who underwent FFR for non-culprit lesions. Patients with negative FFR underwent subsequent OCT and were then further segregated according to whether or not a high-risk TCFA was identified.
Strikingly, in more than 25 percent of all FFR-negative patients, the so-called nonischemic patients, had high-risk plaques carrying TCFAs and those lesions had a significant increase (HR 4.7) in target-lesion related MACE as compared to patients without TCFA at 1.5 years.
In the case of the CLIMA study, investigators only evaluated proximal LAD for 1,000 ACS and stable angina patients. The result, published in the European Heart Journal in 2019, revealed that the OCT-defined high risk plaque features, minimal lumen area (MLA) <3.5mm2, fibrous cap thickness <75μm, lipid arc >180°, and presence of macrophages were all associated with 1-year MACE.
Stone emphasized that for the past 10 years, cardiologists secured much evidence for assessing the risk of vulnerable plaque that gives rise to future adverse cardiovascular events, and that the “time is right” to reconsider the importance of vulnerable plaques.
Park continued with treatment strategies for vulnerable plaques. Since FFR has become popular, functionally insignificant lesions were deferred more for optimal medical treatment (OMT) and showed excellent prognosis. Meanwhile, non-culprit lesions with vulnerable plaque features showed significantly higher event rates similar to culprit lesions. Here, Park focused on the treatment of functionally insignificant vulnerable plaque.
The STABLE trial published in the Journal of American College of Cardiology in 2016 on 300 patients found that rosuvastatin treatment stabilized lesion-specific, local plaque vulnerability with a percentage decrease in NC and frequency of VH- and OCT-TCFAs, as well as decreased plaque volume in non-culprit coronary lesions..
However, because of no significant primary endpoint differences between rosuvastatin 40mg and rosuvastatin 10mg, researchers implied no dose-dependent plaque regression, which may indicate limitations of optimal medical therapy (OMT).
Current guidelines only recommend ischemia-guided revascularization, thus non-ischemia producing lesion is usually treated by optimal medical treatment. However, half of the clinical events occurred at sites with functionally non-significant stenoses prior to becoming a culprit lesion and no data regarding appropriate treatment for functionally insignificant stenosis with vulnerable characteristics exist.
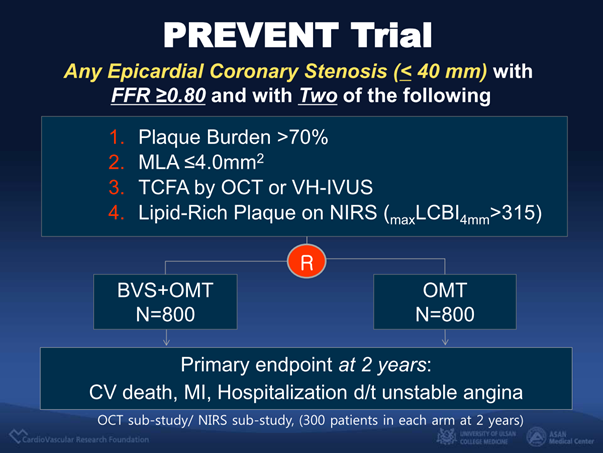
The PREVENT trial therefore focused on the question of whether BVS/DES can stabilize plaque vulnerability that could prevent future events of functionally insignificant lesions.
According to Park, investigators are planning to enroll 1,600 patients with functionally insignificant lesions but with more than two features of vulnerable plaque, such as plaque burden >70%, MLA ≤4.0mm2, TCFA by OCT or VH-IVUS, or lipid rich plaque by NIRS (maxLCBI4mm>315).
Patients will be randomized into either BVS/DES or OMT arms and followed-up in respect to the incidence of composite cardiovascular death, nonfatal myocardial infarction, or unplanned rehospitalization due to unstable angina for two years.
“The PREVENT trial has currently enrolled more than 1,300 patients,” Park said. “The anticipated results may change the treatment paradigm of coronary artery disease.”
Edited by

Mineok Chang, MD
Vuno Inc, Korea (Republic of)