
The use of fractional flow reserve (FFR) or instantaneous wave-free ratio (iFR) in the assessment of coronary lesions in patients with severe aortic stenosis (AS) remains controversial.
 Nils Johnson, MD (UT Health, Texas, USA) highlighted some of the main takeaways from published studies such as ACTIVATION, and ongoing studies such as NOTION-3, FAITAVI that set the scene for discussion during a session at TCTAP Virtual 2021.
Nils Johnson, MD (UT Health, Texas, USA) highlighted some of the main takeaways from published studies such as ACTIVATION, and ongoing studies such as NOTION-3, FAITAVI that set the scene for discussion during a session at TCTAP Virtual 2021.
While noting incoming data from future randomized control trials, Johnson looked at data from a large-scale registry that looked at the FFR readings in 133 lesions before and after TAVI. The registry showed that lesions with high FFR value tend not to change after TAVI while a small number of lesions in the “grey zone” pre-TAVI became significant after valve replacement.
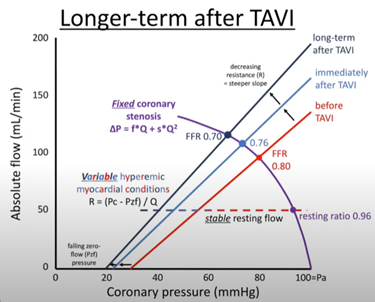
Johnson shared insights on the coronary physiology of severe AS patients and the changes that occur immediately after TAVR and in the longer term after resolution of the myocardial hypertrophy. In the heart AS patients, left ventricular (LV) end-diastolic pressure was high. Pressure in the microvascular bed of LV was also higher than in a heart without AS. Therefore, the flow-pressure curve (absolute flow/coronary pressure) was less steep, which signified increased resistance in microvascular circulation. After the correction of high-pressure gradient with TAVR, immediate changes occurred in the microvascular bed in LV, pushing the flow-pressure curve to a steeper position (rotating counterclockwise). In coronary lesions with same degree of stenosis, a drop in microvascular resistance led to a drop in FFR level after TAVI. Interestingly, there was an interaction between baseline FFR and changes in FFR after TAVI. The FFR levels in significant lesions (baseline FFR <0.8) were more likely to decrease after TAVI than in non-significant lesions (FFR >0.8). On the other hand, resting index remained relatively stable before and after TAVI. Johnson ended the session with final notes on the role of angiographic-based FFR such as QFR and CT FFR in patients with severe aortic stenosis.
QFR, FFRCT improcision increase in AS
Edited by
Yong-Hoon Yoon, MD
Ulsan City Hospital, Korea (Republic of)