
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-103
Presenter
Igor V. Buzaev
Authors
Igor V. Buzaev1, Gulchachak Khalikova1, Tagir Aminov2, Vladimir Plechev1, Irina Evgenievna Nikolaeva2, Almira Davletbaeva3
Affiliation
Bashkir State Medical University, Russian Federation1, Republican Cardiology Center, Russian Federation2, Republic Heart Centre, Russian Federation3,
View Study Report
TCTAP C-103
OTHER - Innovative Devices and Futuristic Therapies
Echonavigator - Hybrid Visualisation Modality for Atrioseptostomia with the Modified Stent in Patient with Severe Pulmonary Hypertension
Igor V. Buzaev1, Gulchachak Khalikova1, Tagir Aminov2, Vladimir Plechev1, Irina Evgenievna Nikolaeva2, Almira Davletbaeva3
Bashkir State Medical University, Russian Federation1, Republican Cardiology Center, Russian Federation2, Republic Heart Centre, Russian Federation3,
Clinical Information
Patient initials or Identifier Number
M14799/20
Relevant Clinical History and Physical Exam
60-year-old female. Symptoms: shortness of breath with little physical exertion, significant decrease in physical activity, independent activity is extremely limited, frequent syncope up to 3 times a week. 2016 - heart cathetherisation: idiopathic pulmonary hypertension. Treatment with sildenafil, opsumit, iloprost. Since 2019 decompensation despite 3 component therapy.
Relevant Test Results Prior to Catheterization
TTE at admit: EDS 3.0, left atrium 3,3 (4,7х3,3), right ventricle 3,8, TAPSE 1,6, right atrium 5,8х4,2, EF(LV) – 58%. Right ventricle hypertrophy. Paradoxical movement of ventricle septum. Enlargement of PA 3,2. Tricuspid regurgitation (++) Vel – 5,0 м/сек. Systolic right ventricle pressure 120, mean right ventricle pressure 50.
Relevant Catheterization Findings
Pulmonary artery wedge pressure 14/5(9), pulmonary artery pressure 143/48(81), right ventricle pressure 132/8(54), right atrial pressure 15/4(9), cardiac output=70х3/1,36х135х(0,96-0,64)=210/59=3,5 l/min.; pulmonary resistance=81-9/3,5= 20 wood.
Interventional Management
Procedural Step
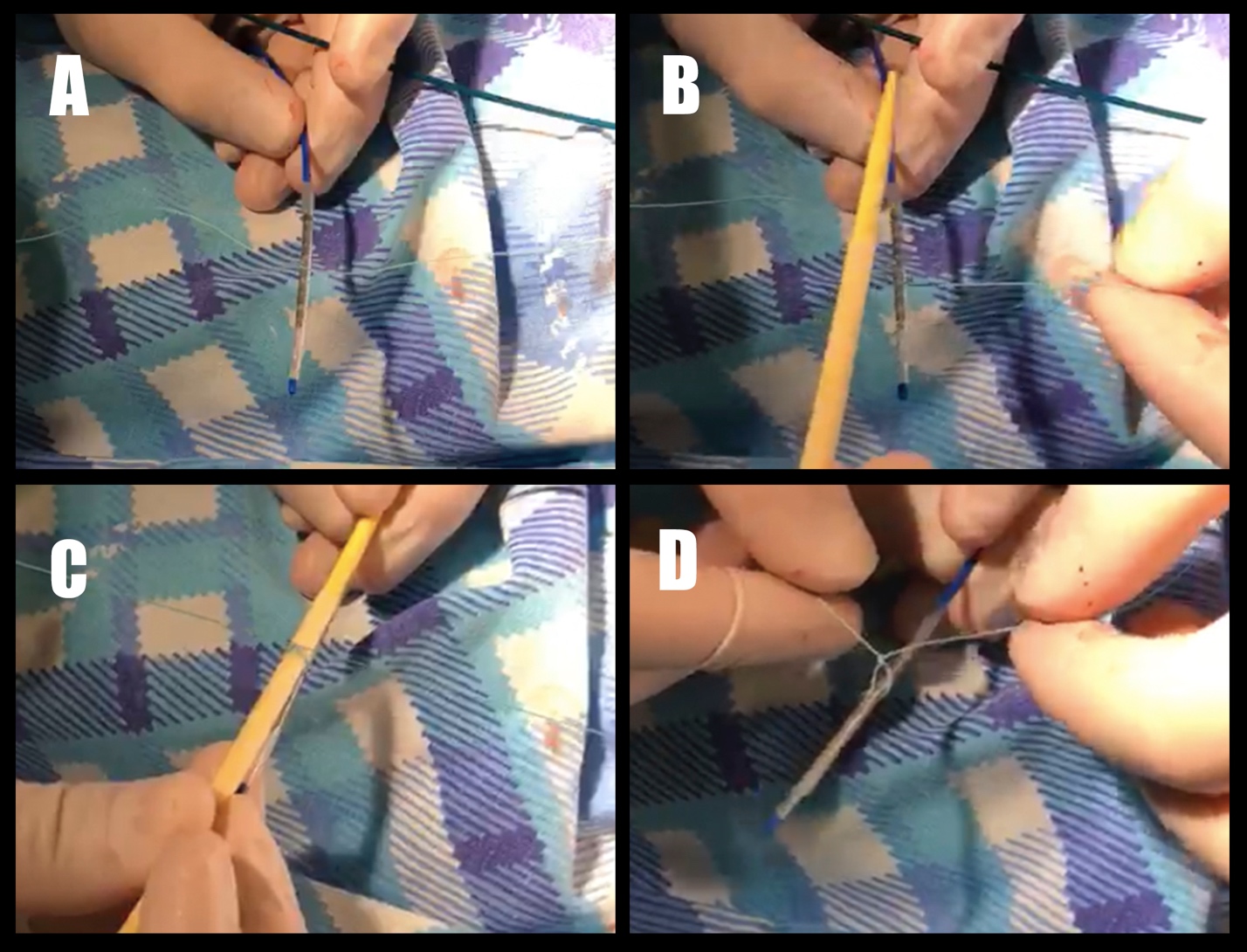
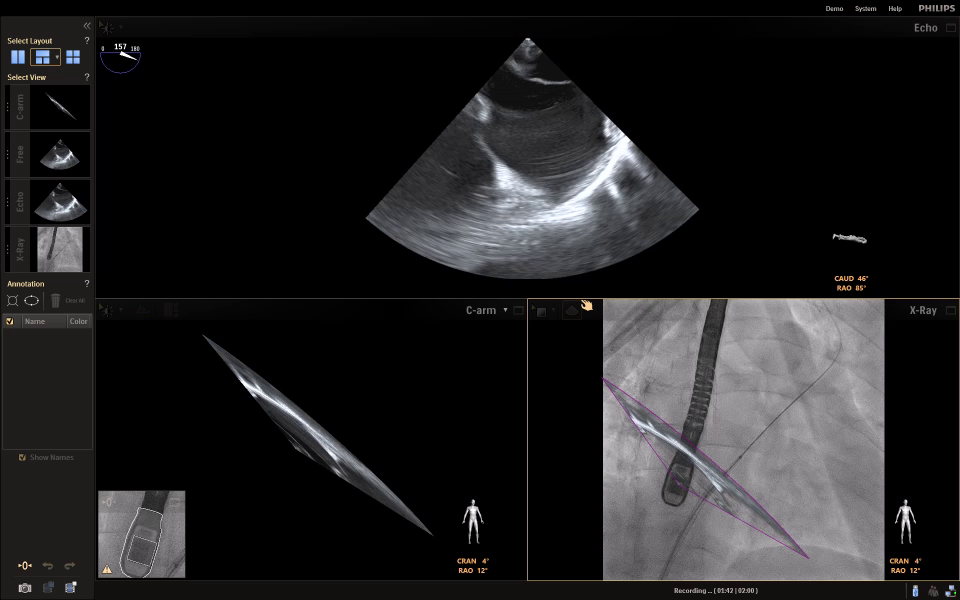
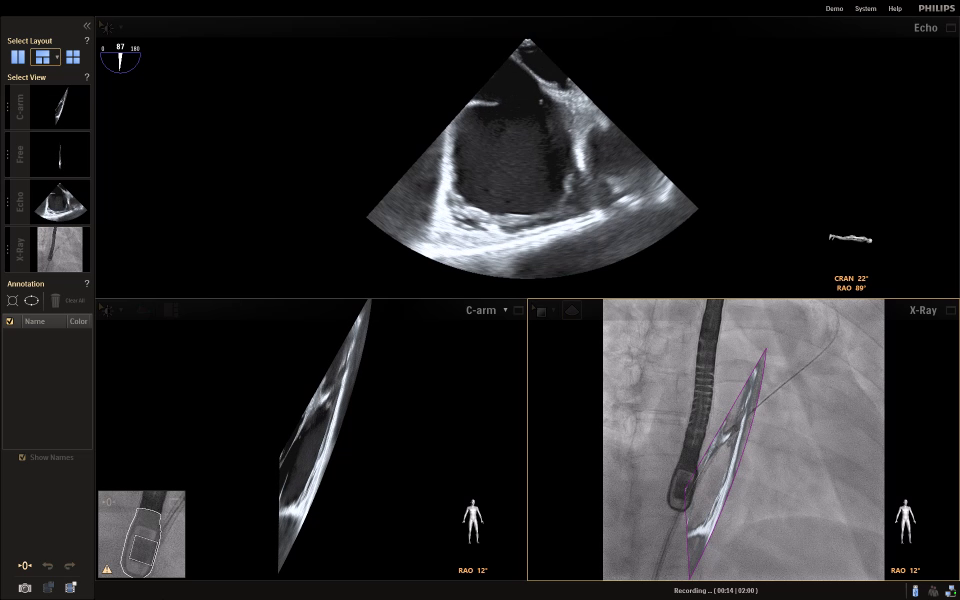
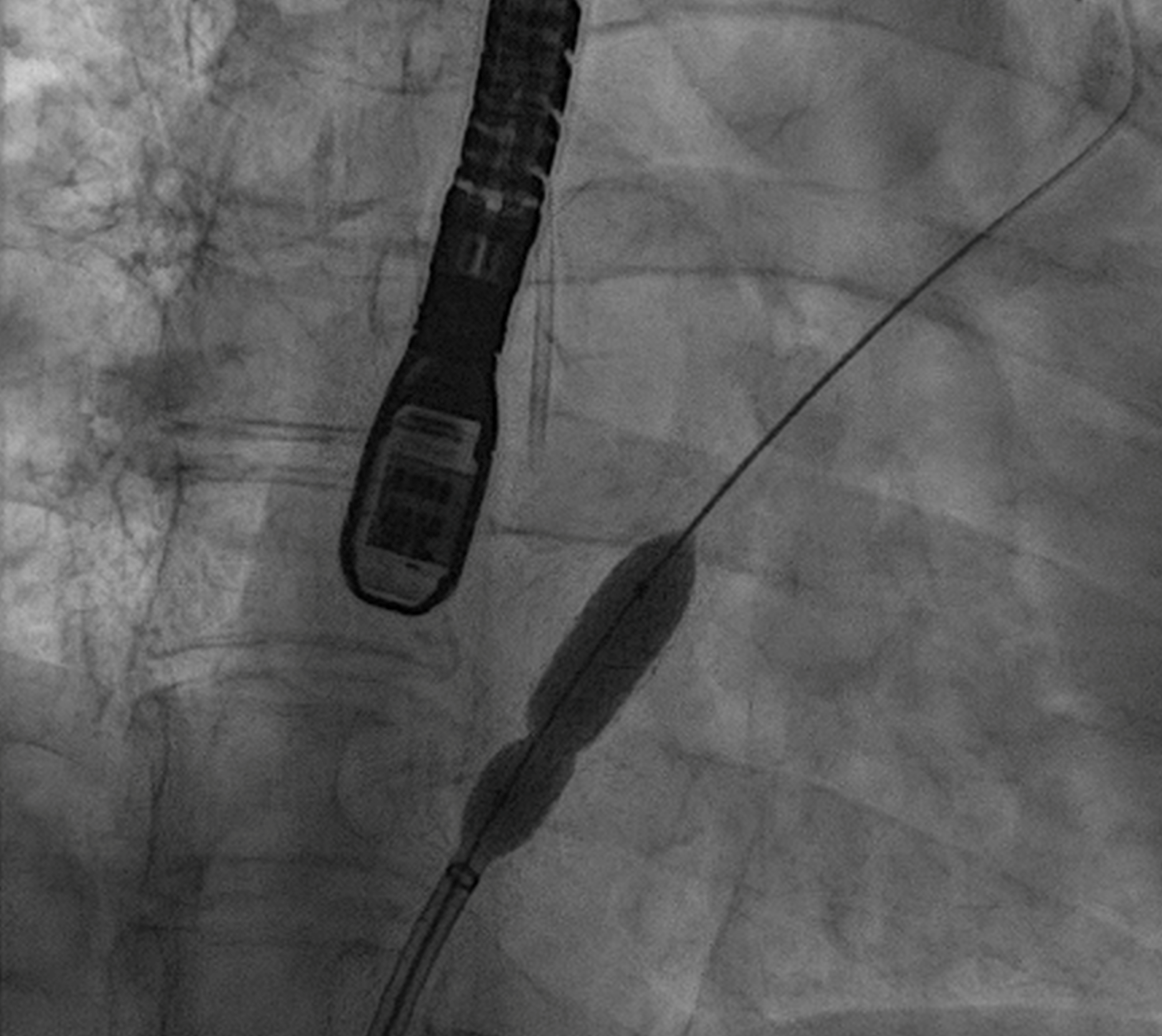
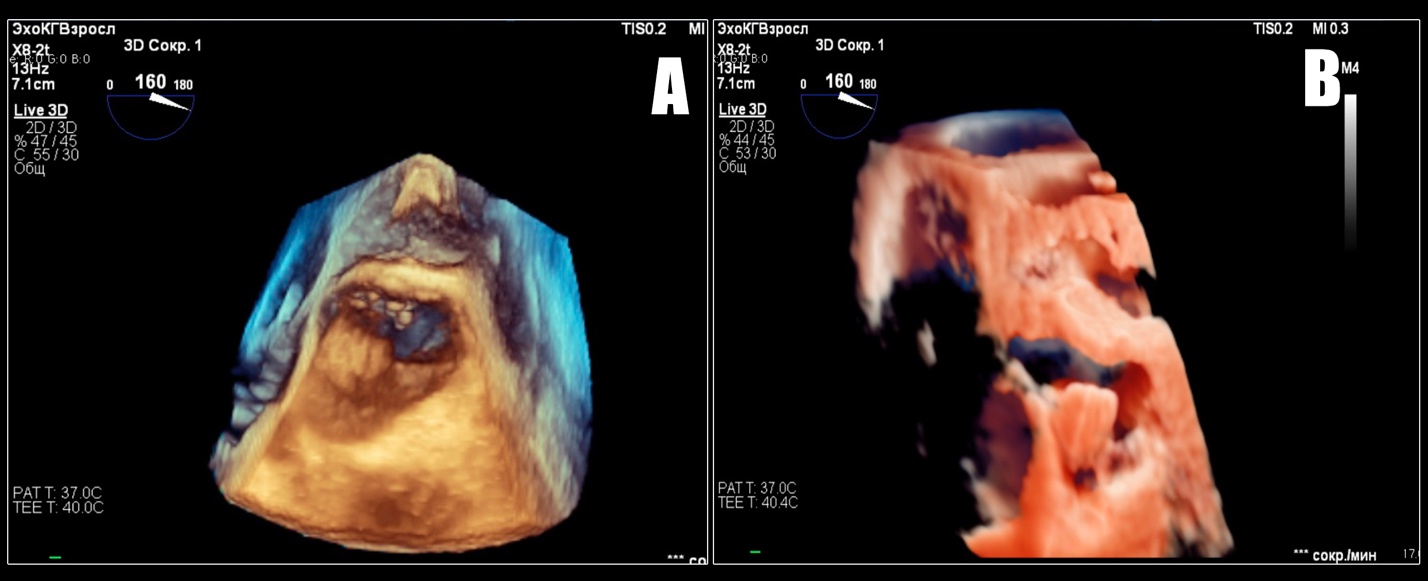
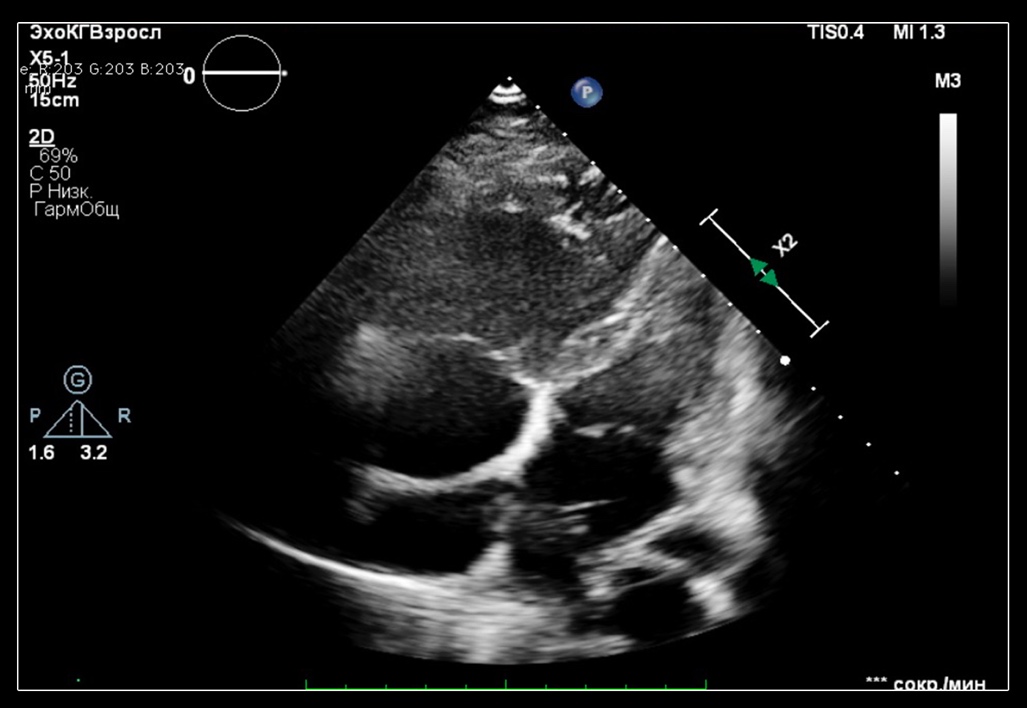
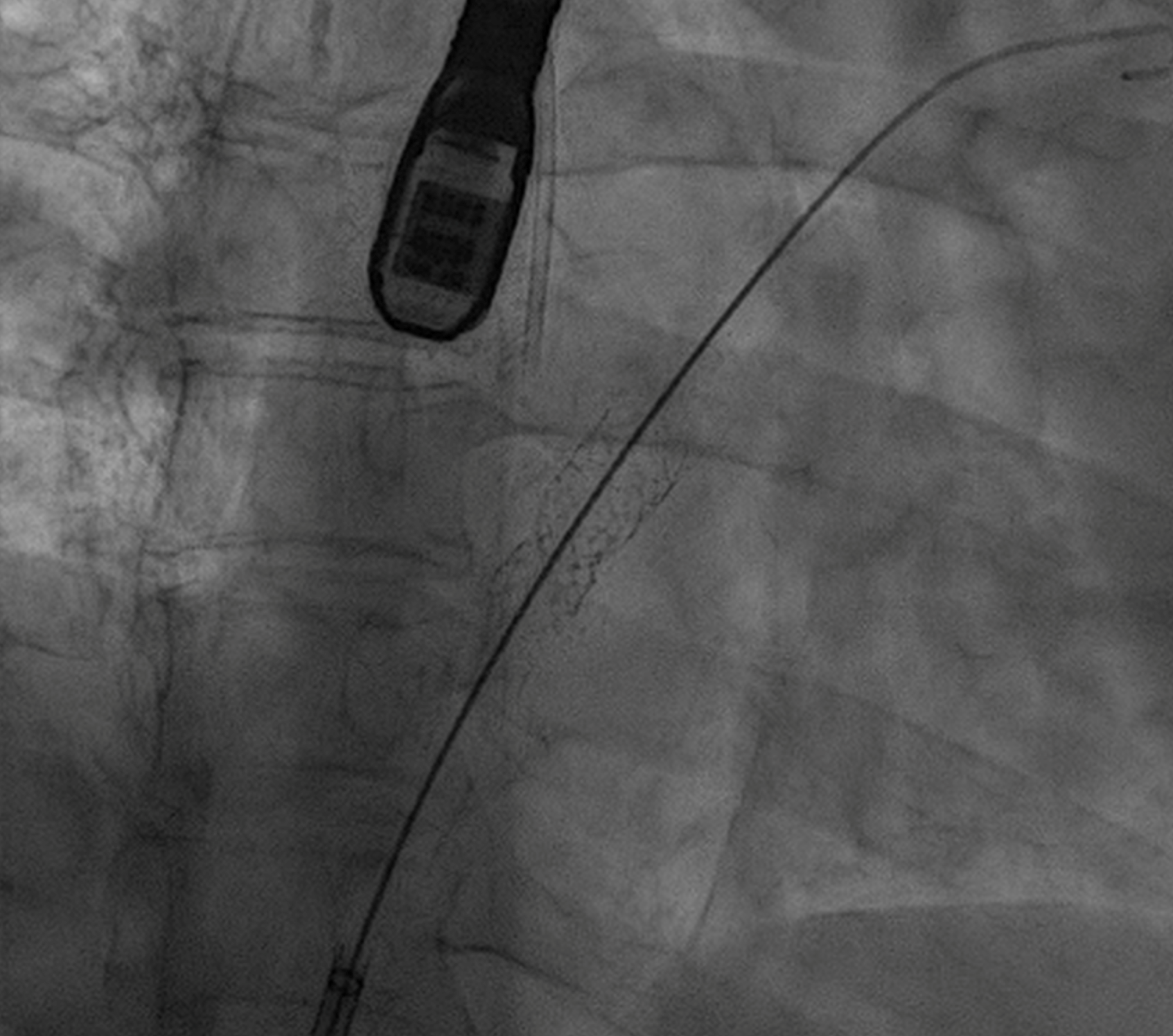
Local anaesthesia. Right femoral vein approach. Fast-Cath™ 8,5. Transseptal puncture under TEE guidance. Balloon predilatation with 6,0x40 balloon at 8 atm. We custom made the special stent for implantation (figure). We made the loop under one of the Palmaz's 9,0х30 start at the middle of the stent. The size of the loop was to make 7 mm diameter of the ring. We used the 6 mm cylinder for that. The loop was over the stent except one strat to limit motion of the loop back and forward. We delivered the stent inside the ASD occluder delivery system to the left atrium. The problem was to put the middle of the stent exactly to the septum. We did not clearly see the septum on fluoro and did not see all the stent on TEE. In this case, Philips Echonavigator system has unique benefit because it combines fluoro and echo real-time picture on the screen. In the picture, you can see the fluoro of the stent and location by the TEE of the atrial septum on one picture. With Echonavigatior system was easy to make positioning of the stent and position and fixation of the stent after deployment was perfect (picture).
TTE post op: EDS LV 4,0 см (left ventricle size increased and left ventricle is decompressed), LA 3,8(4,9х3,8); right ventricle size decreased 3,3; TAPSE 2,0; right atrium size decreased 5,2х3,9; EFLV (increased) 65%. Right to left shunt via stent 6 mm.
Three months follow-up dramatic improvement. No syncope.
TTE post op: EDS LV 4,0 см (left ventricle size increased and left ventricle is decompressed), LA 3,8(4,9х3,8); right ventricle size decreased 3,3; TAPSE 2,0; right atrium size decreased 5,2х3,9; EFLV (increased) 65%. Right to left shunt via stent 6 mm.
Three months follow-up dramatic improvement. No syncope.
Case Summary
1. Atrioseptostomia with 6 mm fenestration is helpful to decompress left ventricle and clinically improve the patients with severe pulmonary hypertension on three component specific therapy. Our case shows the absence of syncope after procedure for 6-month follow-up.2. One of the problems during this procedure is the difficulty to make good positioning of the stent because we see the septum on TEE, but the stent looks like point or short section on TEE. We see the stent on fluoro, but do not see the septum there.
3. Hybrid modality using Philips Echonavigator system is the solution because it combines benefits of echo and fluoro on one screen realtime and it is an irreplaceable tool in this procedure.
3. Hybrid modality using Philips Echonavigator system is the solution because it combines benefits of echo and fluoro on one screen realtime and it is an irreplaceable tool in this procedure.