
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-091
Presenter
Yen-Liang Lin
Authors
Yen-Liang Lin1, Jen-Kuang Lee2
Affiliation
National Taiwan University Hospital Hsinchu branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
View Study Report
TCTAP C-091
ENDOVASCULAR - Peripheral Vascular Disease and Intervention
Endovascular Intervention for Acute Superior Mesenteric Artery Occlusion with Multi-discipline Modalities
Yen-Liang Lin1, Jen-Kuang Lee2
National Taiwan University Hospital Hsinchu branch, Taiwan1, National Taiwan University Hospital, Taiwan2,
Clinical Information
Patient initials or Identifier Number
ZKL, 1546488
Relevant Clinical History and Physical Exam
An 85-year-old man presented with acute abdominal pain for 1 day. He had atrial fibrillation (AF), but he did not take medication for it. The physical exam revealed soft and flat abdomen without localized tenderness or guarding.

Relevant Test Results Prior to Catheterization
Lab data showed anemia (HB 8.8 g/dL), no leukocytosis, normal value of amylase and lipase, but elevated D-dimer (2.08 ug/mL) and lactic acid level (4.79 mmol/L).KUB revealed no free air accumulation in the abdomen. Abdominal CT reported occlusion of superior mesenteric artery with ischemic and edematous changes of small bowel.
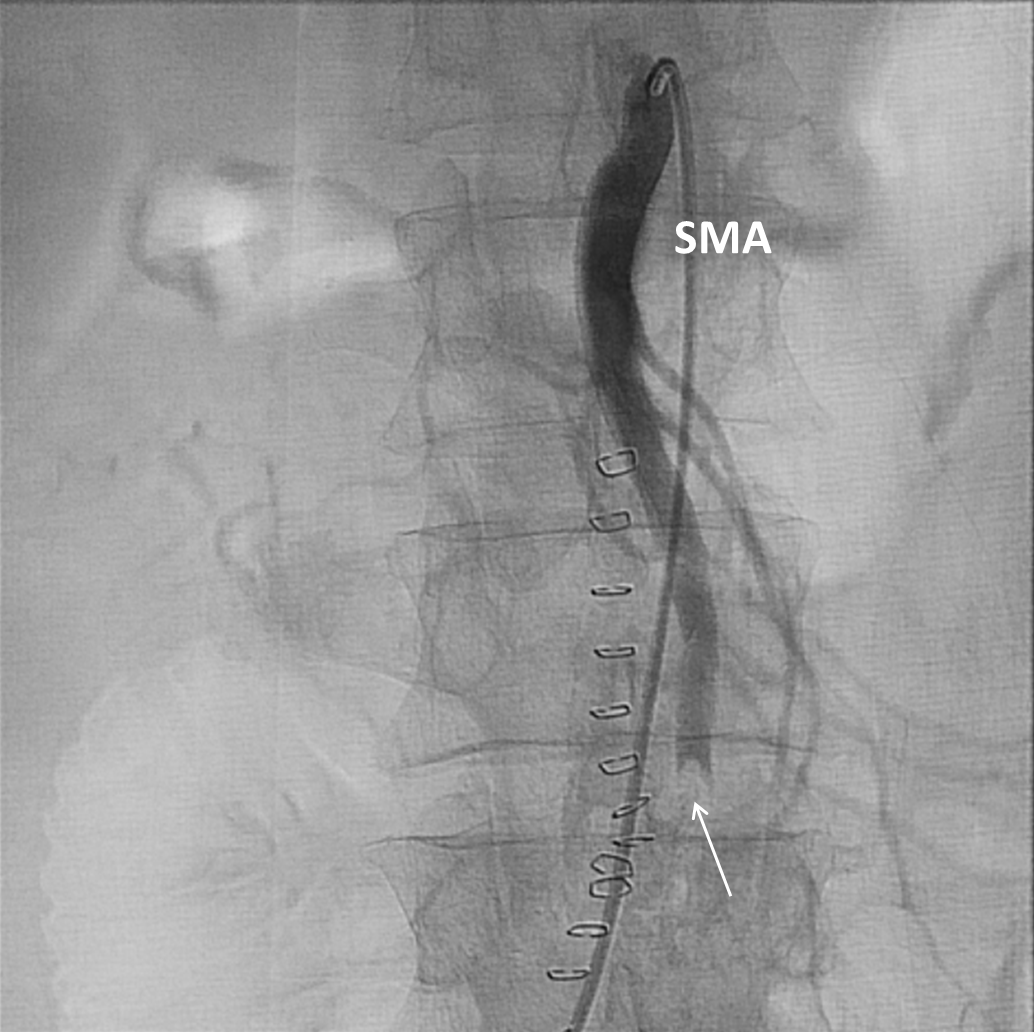
Relevant Catheterization Findings
Total occlusion with large thrombi burden at one of the branch of superior mesenteric artery.
Interventional Management
Procedural Step
1st Intervention:
1. Engage guiding catheter "COOK FLEXOR TUOHY BORST INTRODUCER 7FR 45cm ANL2" to SMA
2. Deliver wire "COOK Hydro wire .014 300cm" to ileo-colic branch
3. Change guiding catheter with "ev3 MARKSMAN CATHETER", and send microcatheter "ev3 Navien 058 Intracranial Support Catheter" to ileo-colic branch
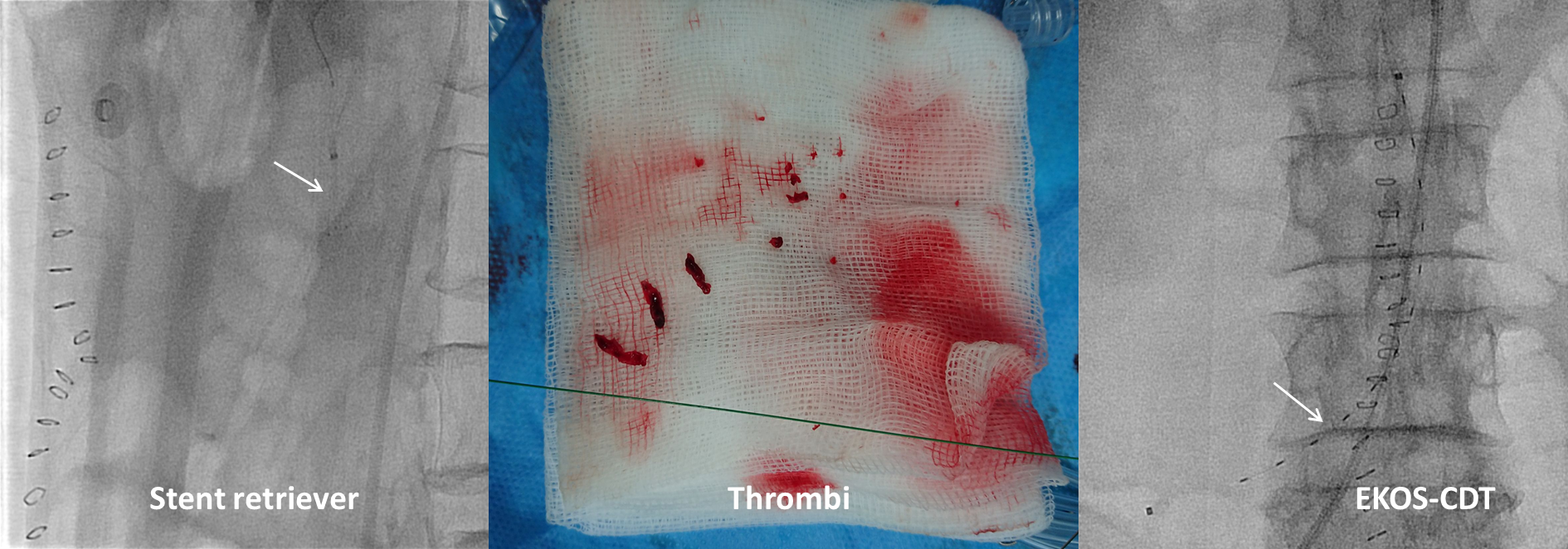
4. Thrombectomy by stent retriever "Abbott " MTI ” Solitaire FR Revascularization Device SRD-4-20", and retrieve much red thrombi
5. Aggrastat infusion for thrombolysis
6. Switch microcatheter with "COOK CXI 2.6 FR 90cm P-NS-0" to ileo-colic branch
7. Thrombosuction by "Vascular Solutions Pronto V4 Extraction catheter 8F", and aspirate much red thrombi
8. Deliver wire "ASAHI Regalia XS1.0-300" to jejuno-ileal branch
9. Angioplasty with balloon catheter "Bard BANTAM α 3X40 MM * 150CM" and "Boston Scientific Coyote OTW 2.5 X 80, 150 cm" to both branches of SMA
10. Implant EKOS to distal SMA and ileo-colic branch for thrombolysis
2nd Intervention (2 days later):
1. Still poor flow with much thrombi in SMA
2. Deliver wire "ASAHI Regalia XS1.0-180" to distal SMA
3. Angioplasty with balloon catheter "Medtronic Euphora Balloon 2*15mm", but still poor flow
4. Thrombosuction by "Vascular Solutions Pronto V4 Extraction catheter 7F" and "Kaneka Thrombuster7F", and aspirate some large red thrombi
5. Still poor flow of SMA after thrombosuction
6. Angioplasty and stent deployment with "BIOTRONIK Pro-Kinetic Energy (CoCr) 3.0*30mm" to distal SMA
7. SMA flow improved a lot
 SMA occlusion aspiration.avi
SMA occlusion aspiration.avi
SMA occlusion final.avi
1. Engage guiding catheter "COOK FLEXOR TUOHY BORST INTRODUCER 7FR 45cm ANL2" to SMA
2. Deliver wire "COOK Hydro wire .014 300cm" to ileo-colic branch
3. Change guiding catheter with "ev3 MARKSMAN CATHETER", and send microcatheter "ev3 Navien 058 Intracranial Support Catheter" to ileo-colic branch
4. Thrombectomy by stent retriever "Abbott " MTI ” Solitaire FR Revascularization Device SRD-4-20", and retrieve much red thrombi
5. Aggrastat infusion for thrombolysis
6. Switch microcatheter with "COOK CXI 2.6 FR 90cm P-NS-0" to ileo-colic branch
7. Thrombosuction by "Vascular Solutions Pronto V4 Extraction catheter 8F", and aspirate much red thrombi
8. Deliver wire "ASAHI Regalia XS1.0-300" to jejuno-ileal branch
9. Angioplasty with balloon catheter "Bard BANTAM α 3X40 MM * 150CM" and "Boston Scientific Coyote OTW 2.5 X 80, 150 cm" to both branches of SMA
10. Implant EKOS to distal SMA and ileo-colic branch for thrombolysis
2nd Intervention (2 days later):
1. Still poor flow with much thrombi in SMA
2. Deliver wire "ASAHI Regalia XS1.0-180" to distal SMA
3. Angioplasty with balloon catheter "Medtronic Euphora Balloon 2*15mm", but still poor flow
4. Thrombosuction by "Vascular Solutions Pronto V4 Extraction catheter 7F" and "Kaneka Thrombuster7F", and aspirate some large red thrombi
5. Still poor flow of SMA after thrombosuction
6. Angioplasty and stent deployment with "BIOTRONIK Pro-Kinetic Energy (CoCr) 3.0*30mm" to distal SMA
7. SMA flow improved a lot
Case Summary
Acute SMA occlusion is risky and catastrophic because this medical emergency leads to ischemic bowel disease. Multi-discipline modalities may be needed to revascularize the occluded SMA without any delay. We successfully performed endovascular intervention with numerous techniques and devices in one patient, including stent retriever (thrombectomy), thrombosuction catheter (thrombosuction), catheter-directed thrombolysis (thrombolysis), and stent deployment. Endovascular intervention provides an effective and safe way to revascularize acute SMA occlusion other than open surgery.