
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-025
Presenter
Mugilan Sundarajoo
Authors
Mugilan Sundarajoo1
Affiliation
National Heart Institute Ijn, Malaysia1,
View Study Report
TCTAP C-025
CORONARY - Bifurcation/Left Main Diseases and Intervention
"Drilling Through History" - A Case of Calcified Left Main Bifurcation Lesion with Rotablation and DK-crush in a Patient with High Bleeding Risk
Mugilan Sundarajoo1
National Heart Institute Ijn, Malaysia1,
Clinical Information
Patient initials or Identifier Number
412690
Relevant Clinical History and Physical Exam
An 82 years old lady with co-morbids of Type 2 diabetes mellitus, hypertension, chronic kidney disease Stage III B presented with chest pain on exertion and reduced effort tolerance for 2 weeks. Angioplasty (DES) to the mid Right Coronary Artery was done in 2018. She was treated as Non ST elevation Myocardial Infarction. Physical examination revealed bilateral base fine end inspiratory crepitations with minimal pitting pedal oedema. Cardiac auscultation revealed dual rhythm with no murmur.
Relevant Test Results Prior to Catheterization
Chest X-ray revealed pulmonary congestion with minimal left pleural effusion. NT Pro-BNP - 3250, Troponin T - 1245. Echocardiography showed an ejection fraction of 38 % with comparatively normal right ventricular function. There was mild mitral regurgitation. ECG showed T inversions over V2- V6.
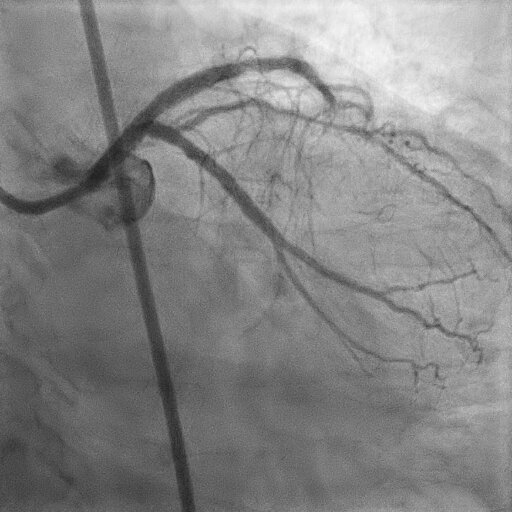
Relevant Catheterization Findings
Left Main Stem - severe distal Left Main Stem diseaseLeft Anterior Descending - Severe ostial to mid disease calcified lesion with Chronic Total Occlusion of distal LeftAnterior DescendingLeft Circumflex - Severe ostial calcified diseaseRight Coronary Artery - Patent stent with mild stenosis over proximal Right Coronary Artery
CABG was offered in view of high Syntax score (38) and concomitant high bleeding risk but the patient opted for high risk PCI.
CABG was offered in view of high Syntax score (38) and concomitant high bleeding risk but the patient opted for high risk PCI.
Interventional Management
Procedural Step
Percutaneous Coronary Intervention to Left Main Stem (LMS) was done via right radial approach.Left coronary (LCX) ostium engaged with 7 FR EBU 3.5. Ostium of LCX was predilated with Sapphire II PRO 1.5 x 15 mm.Rotablation done into LMS into LCX with Rotablator- 1.5 burr at 160000 rpm - 170000 rpm.Proximal LCX was further predilated with Sapphire II NC 2.5 x 15 mm.Sapphire II NC 2.5 x 15 mm was used to predilate Left anterior descending artery (LAD) at 12 atm.Subsequently, predilation of LCX done with Sapphire II NC 2.5 x 15 mm at 12 atm.Rotablation to LAD done using 1.5 Burr at 160000 rpm - 170000 rpm.DK CRUSH technique was used for the stenting of LMS - LAD - LCXPredilatation of LAD with 2.5 x 12 mm NC Sapphire done upto 24 atm at ostial LAD.Stent was deployed over mid to ostial LCX with Xience Alpine 2.75 x 38 mm.The stent was then crushed with Sapphire 2.5 NC at 12 atm. First kissing ballon inflation done using Sapphire II NC 3.0 x 15 mm in LCX and Sapphire II NC 3.5 x 12 mm in LAD.Stent was deployed upto mid of LAD extending to Left Main Stem with Xience Alpine 3.5 x 28 mm then post dilated Left Anterior Descending 3.5 x 12 mm upto 14 atm. Second kissing balloon inflation was done using Sapphire II NC 3.0 x 15 mm in LCX and Sapphire II NC 3.5 x 18 mm in LAD.Final POT done with NC Rise 4.0 x 15 mm at 14 atm.Good end results, TIMI 3 Flow with no complications. Patient has been well with no major adverse cardiovascular event or bleeding for the last 10 months post procedure.
 faezah 1.avi
faezah 1.avi
faezah 2.avi
Case Summary
Coronary intervention of calcified bifurcation disease involving the left main stem in a high bleeding risk patient is truly a challenge. Rotational atherectomy is an established technique for effective modification of these lesions prior to conventional angioplasty and stent implantation. The combination of Rotablation and DES in calcified coronary artery lesions has a very good angiographic result with satisfactory clinical outcome. DK crush has been proven to be the 'real deal' in bifurcation lesions.