
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-044
Presenter
Hyunsu Kim
Authors
Hyunsu Kim1
Affiliation
On Hospital, Korea (Republic of)1,
View Study Report
TCTAP C-044
CORONARY - Chronic Total Occlusion
Microcatheter (Cosair) Assisted Penetration of Long Standing CTO Lesion of LAD ostium
Hyunsu Kim1
On Hospital, Korea (Republic of)1,
Clinical Information
Patient initials or Identifier Number
15245060
Relevant Clinical History and Physical Exam
He had a history of long standing diabetes mellitus. In 2015, during preoperative evaluation for stomach cancer, he got the coronary angiography due to chest pain. Coronary angiography showed CTO at LAD ostium, intermedius branch and diffuse thrombotic lesion at RCA with Gr 3 collaterals to LAD. He received medical treatment only after gastrectomy. In July 2020, He got the PCI at RCA ostium due to new developed NSTEMI. After 3 months, he admitted for second staged PCI for LAD CTO lesion.

Relevant Test Results Prior to Catheterization
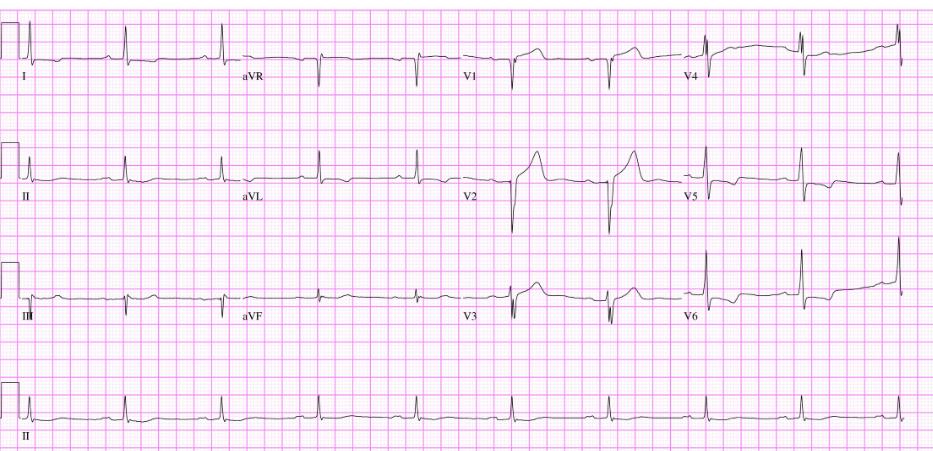
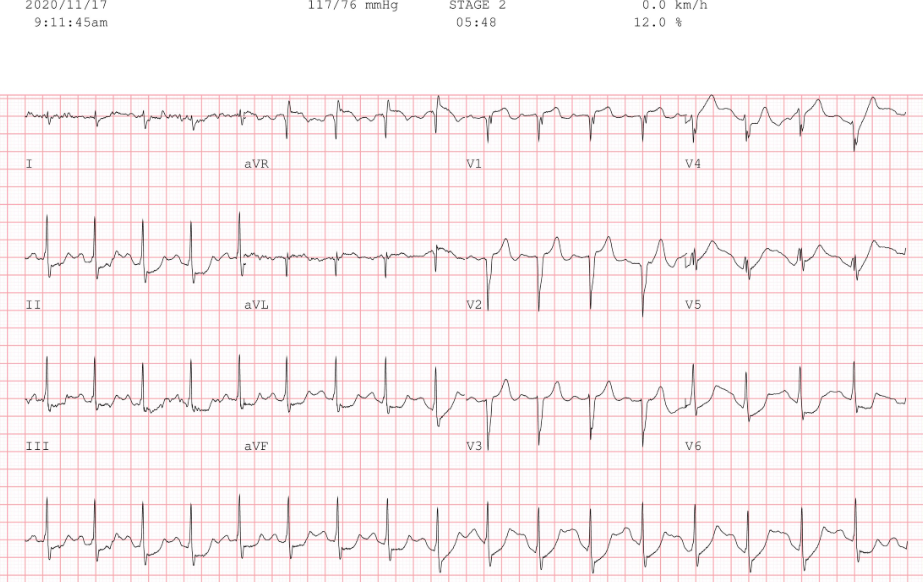
His electrocardiogram showed normal sinus rhythms and poor R progression at precordial leads and ST depression at V5, 6. Exercise stress test showed ST depression at stage 2. Echo cardiogram showed preserved LV ejection fraction without significant wall motion abnormalities. Cardiac enzymes were within normal limits.
Relevant Catheterization Findings
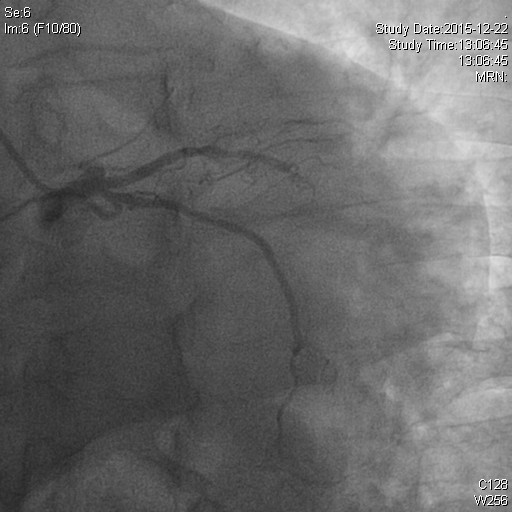
Coronary angiogram showed patent previous stents at proximal and distal RCA and collaterals to mLAD bifurcation level. Left angiogram showed total occlusion at LAD ostium without stump, some spotty calcifications to mLAD and total occlusion at intermedius branch.
 2.avi
2.avi
3.avi
7.avi
Interventional Management
Procedural Step
Rt. radial artery and Rt. femoral artery were punctured. Via Rt. radial diagnostic JR 5Fr catheter was used for collateral angiogram. First, negotiation was tried using 014 Fielder XT with microcatheter support. The Fielder wire progressed mid portion of CTO, however, the wire progressed wrong direction due to angulation at bifurcation area. I changed the wire into Gaia 3 wire for making a different channel for true direction. After changing direction of wire, pushed the microcatheter deeply and change the wire into Fielder again. After that, I could penetrate CTO lesion successfully. Unfortunately, preballooning with 1.0mm x 15mm size couldn't pass through the lesion due to heavy calcification and tight stenosis although support with Guidelines. I used Corsair microcatheter for progress and expansion of tight lesion. I rotated Cosair several times, then Cosair could pass through the lesion. After expanding tight lesion, 1.0 mm sized preballoon could pass the lesion and preballooing was done using 1.5 mm, 2.5 mm sized serially. After ballooning 2 stents (Onyx 3.0 mm x 34mm. Onyx 3.0x 30mm) were deployed. Final angigram showed good flow.

17.avi
50.avi
Case Summary
This case is successful negotiation of severely tight and hard calcified long standing CTO lesion that couldn't pass using the smallest 1.0mm sized conventional pre-balloon. The lesion could be negotiated using rotation of Cosair microcatheter technique.