
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-023
Presenter
Khairul Shafiq Ibrahim
Authors
Khairul Shafiq Ibrahim1, Abdul Wahab Undok2, Rizmy Najme Khir3, Raja Ezman Raja Shariff4, Sazzli Kasim1
Affiliation
Universiti Teknologi MARA (UiTM), Malaysia1, Kpj Rawang Specialist Hospital, Malaysia2, Ara Damansara Medical Centre, Malaysia3, Hospital Universiti Teknologi MARA (UiTM), Malaysia4,
View Study Report
TCTAP C-023
CORONARY - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
The Finecross of the Day - A Case of Percutaneous Intervention to Anomalous Right Coronary Artery
Khairul Shafiq Ibrahim1, Abdul Wahab Undok2, Rizmy Najme Khir3, Raja Ezman Raja Shariff4, Sazzli Kasim1
Universiti Teknologi MARA (UiTM), Malaysia1, Kpj Rawang Specialist Hospital, Malaysia2, Ara Damansara Medical Centre, Malaysia3, Hospital Universiti Teknologi MARA (UiTM), Malaysia4,
Clinical Information
Patient initials or Identifier Number
AB
Relevant Clinical History and Physical Exam
Mr AB is a 78 years old man with type 2 diabetes and dyslipidaemia. He actively cycles 80km per week and regularly does a 10km run. He presented with a one-month history of progressively reduced effort tolerance and chest pain on exertion. On examination, he is generally well with normal vital signs. Cardiovascular and respiratory examinations were unremarkable.
Relevant Test Results Prior to Catheterization
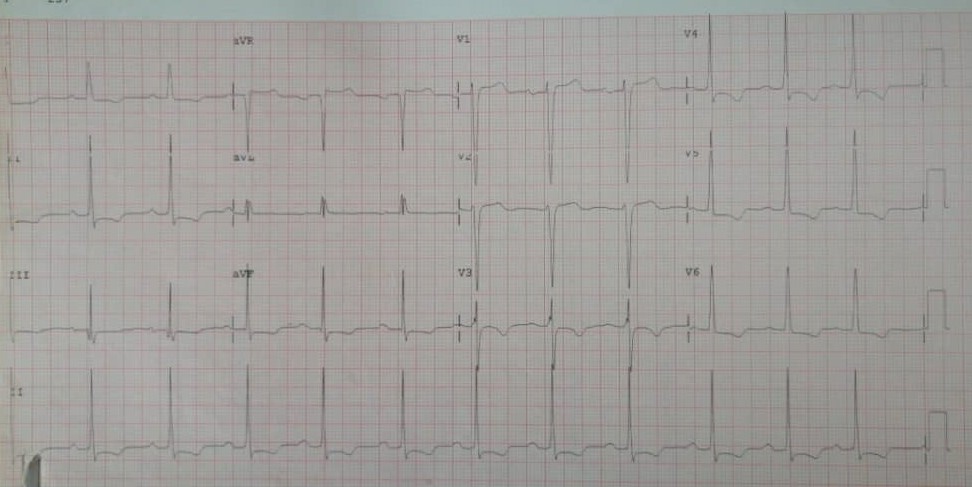
His haemoglobin was 14.4 g/dL, low density lipoprotein of 4.0 mmol/L, eGFR of 64ml/min/1.73m2 and HbA1C of 6.9%. His electrocardiogram showed left ventricular hypertrophy with diffuse ST segment depression and AVR ST elevetion. Echocardiogram showed left ventricular ejection fraction of 48% with hypokinetic over mid to apical posterior, anterior, lateral and septal.
Relevant Catheterization Findings
Diagnostic catheterisation showed diffuse disease in left anterior descending artery (LAD) with severe stenosis at the mid LAD and diffuse disease at distal left circumflex (LCx). There are collateral vessels to the right coronary artery (RCA) from the septal branch. The RCA arose from left coronary cusp, diffusely disease with chronic total occlusion at distal RCA.
 pa caudal.wmv
pa caudal.wmv
lat.wmv
lao cra r.wmv
Interventional Management
Procedural Step
Trial of engagement to the anomalous RCA with JR 3.5 6Fr andAL0.75 6Fr via right radial artery was unsuccessful. Using LAO view, we manage to bring the JL 4.0 6Fr close to the ostium of anomalous RCA. Sion blue wire was used to wire down from outside to the cap of RCA CTO. Finecross microcatheter was inserted into RCA over the sion blue wire to act as an anchor. With finecross support, the JL guiding was successfully pushed and engaged in a power position. Dual puncture techniques was used. JL 3.5 diagnostic catheter was engaged into the left system. Finecross was advanced to the cap of CTO. Wire exchanged to Fielder XTR. The CTOlesion was successfully crossed with Fielder XTR. Finecross was successfully advanced across the CTO lesion. Wire exchanged back to sion blue. Lesion was predilated with 2.0/12 and 2.5/15 semi-compliance balloon at the mid and distal RCA. The proximal lesion was predilated with NC 3.5/15. 2.75/38 stent and3.5/20 stent was deployed to the mid RCAand proximal RCA respectively. Post dilatation was performed to the mid and proximal RCA stent with NC 3.5 and NC 3.75 respectively.
MOVIE-0005.wmv
MOVIE-0007.wmv
MOVIE-0040.wmv
Case Summary
In an anomalous right coronary artery arisen from left coronary cusp intervention, Judkins left 4.0 guiding catheter via right radial artery approach can be used. Adjunct use of microcatheter can be attempted to provide support for catheter engagement into coronary artery.