
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-087
Presenter
Osama Shoeib
Authors
Osama Shoeib1, Hazem Mamdouh Warda2
Affiliation
Tanta University Hospital, Egypt1, Alhyatt Heart and Vascular Center, Egypt2,
View Study Report
TCTAP C-087
ENDOVASCULAR - Carotid & Neurovascular Intervention
Transradial carotid artery stenting complicated with neck hematoma, conservative is a valid option!
Osama Shoeib1, Hazem Mamdouh Warda2
Tanta University Hospital, Egypt1, Alhyatt Heart and Vascular Center, Egypt2,
Clinical Information
Patient initials or Identifier Number
FA
Relevant Clinical History and Physical Exam
Male patient 56 years old, he is diabetic and hypertensive with previous history of ischemic heart disease that was treated with multiple percutaneous coronary intervention (PCI), the patient experienced an attack of transient ischemic attack (TIA) three weeks ago.
Relevant Test Results Prior to Catheterization
carotid doppler was done and revealed right internal carotid artery stenosis with systolic flow velocity of 300cm/sec, that was confirmed by a computational tomography (CT)scan.
Relevant Catheterization Findings
The patient was discussed at our heart team meeting and percutaneous carotid artery stenting was advised given the high cardiovascular risk for the carotid artery endarterectomy.
Interventional Management
Procedural Step
Right radial access waschosen with regular 6 fr sheath, a guiding catheter XB 3.5 was introduced tothe aortic arch, then guide wire withdrawn to allow the catheter to bend onitself with slight rotation we directed the catheter tip toward thebrachiocephalic trunk then a Terumo stiff 300 cm wire was advanced toward the CCA,with the help of road map the wire was advanced to good distal portion of the ECA.

Case Summary
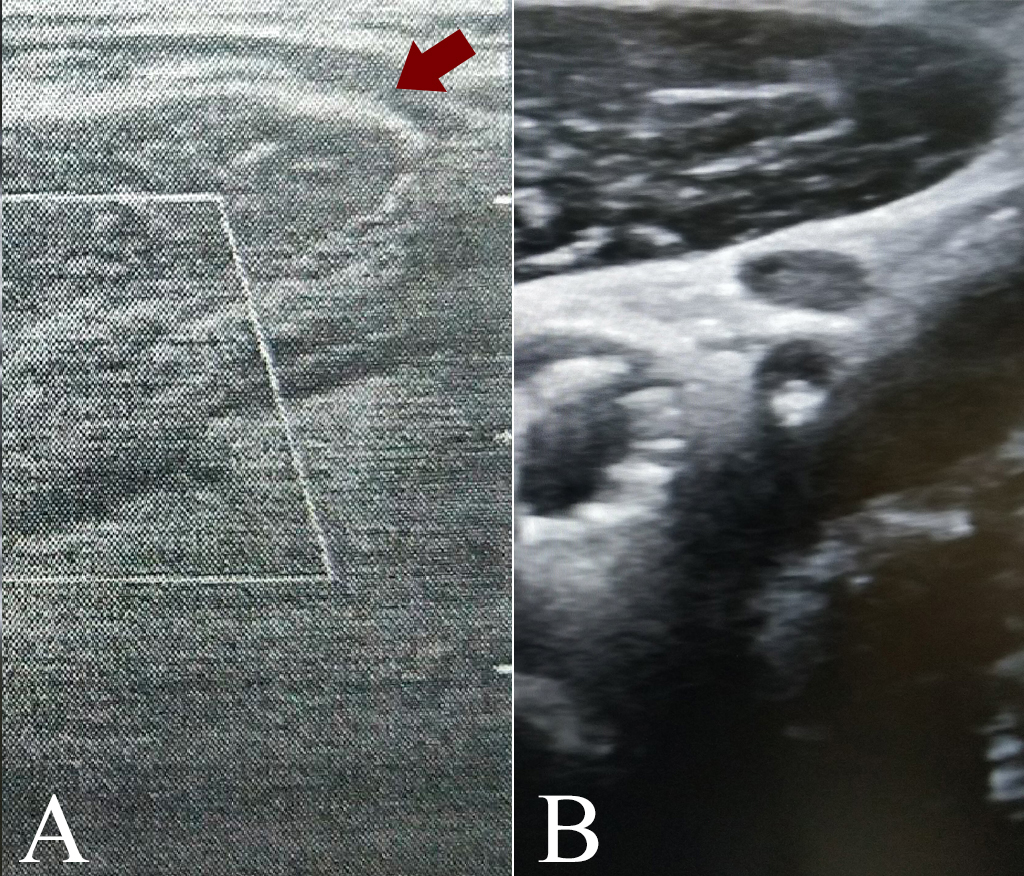
Usage of stiff Treumo wires in carotid intervention showed be used with extreme caution and under strict maneuvers to reduce the perforation possibilities and may be replaced with atraumatic tip wires that may provide more safety to the procedures.Even if perforation happens US availability and operator's familiarity with rapid scanning is crucial to help complication definitions and diagnosis, also small hematomas can be conservatively managed and followed up and reserve coiling for large branches and large hematomas, but coiling materials should always be available and ready to use.