
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-074
Presenter
Wongsakorn Luangphiphat
Authors
Wongsakorn Luangphiphat1, Jutatip Na Witayanan2, Purich Surunchupakorn3, Thamarath Chantadansuwan3, Wirash Kehasukcharoen3
Affiliation
Chulabhorn Hospital, Thailand1, central chest institution of Thailand, Thailand2, Central Chest Institute of Thailand, Thailand3,
View Study Report
TCTAP C-074
CORONARY - Complications
Uncommon Jailed Wire Complication
Wongsakorn Luangphiphat1, Jutatip Na Witayanan2, Purich Surunchupakorn3, Thamarath Chantadansuwan3, Wirash Kehasukcharoen3
Chulabhorn Hospital, Thailand1, central chest institution of Thailand, Thailand2, Central Chest Institute of Thailand, Thailand3,
Clinical Information
Patient initials or Identifier Number
45
Relevant Clinical History and Physical Exam
A 45-year-old male, ex-smoker, HT, DLP. Presented with inferior wall STEMI which CAG diagnosed TVD underwent PPCI to RCA 9 months ago. After staging PCI to LCx he was arranged for elective PCI on this admission.
Relevant Test Results Prior to Catheterization
Laboratory showed Hct 44%, Cr 0.93 mg/dL, eGFR 99ml/min/1.73 m2, LDL 74 mg/dL and HDL 40 md/dL.
Relevant Catheterization Findings
LAD showed diffuse 70-80% lesion from proximal to mid LAD with a tight lesion at proximal DG1. PCI to both LAD and DG1 was planned with provisional T stent over the bifurcation. Sion Blue and Sion wire were placed in LAD and DG1 respectively. After stented the mid LAD and DG1, a 3.0/34 mm DES was deployed from LAD ostium to overlap with mid LAD stent. Angiogram post stenting showed good flow in both LAD and DG1, but the wire in DG1 was unable to be pulled out.
 1.avi
1.avi
2.avi
3.avi
4.avi
5.avi
Interventional Management
Procedural Step
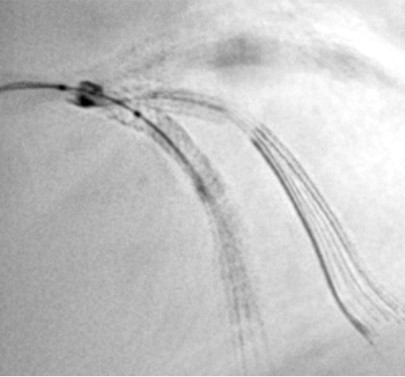
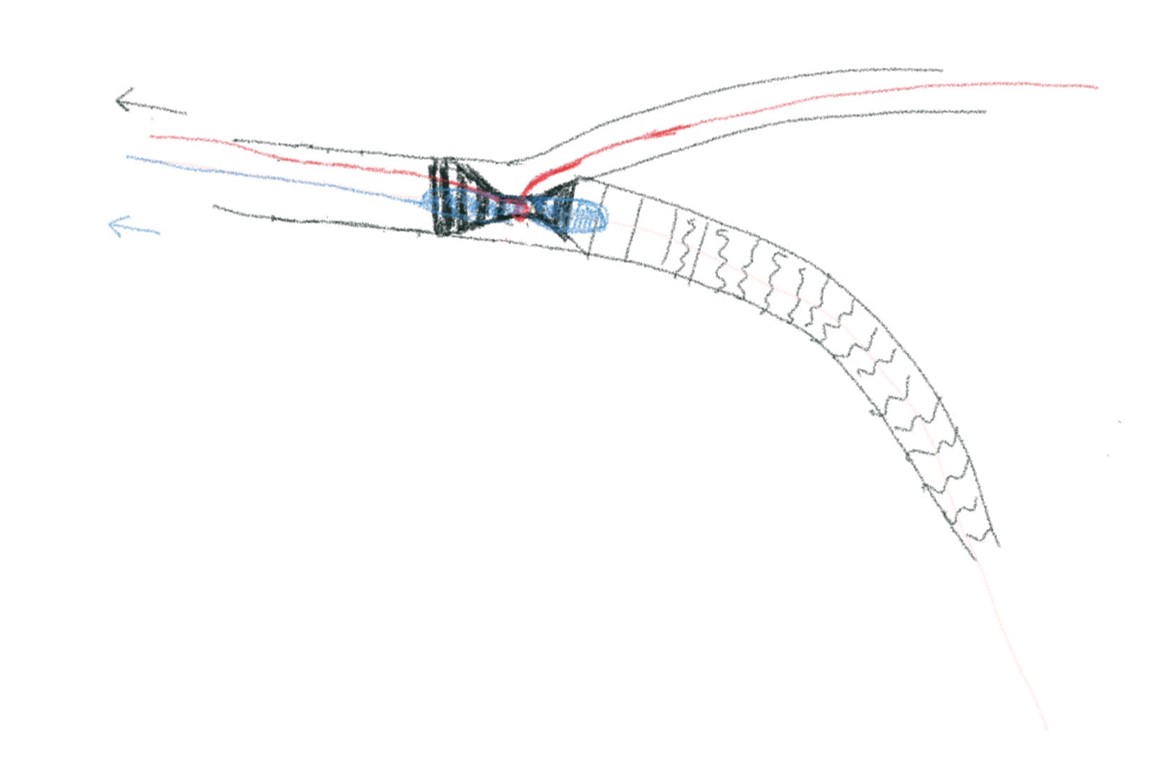
Attempts to remove entrapped side branch wire with various devices and techniques were failed. Stent enhanced cinefluorography showed severely deformed proximal part of stent where it was squeezed by pulling side branch wire loop. Planned to remove both entrapped wire and deformed stent together but there's no specific device for this purpose.
6.avi
9.avi
Case Summary
Beware the angle and curve of the wire at the lesion site after ballooning and before stenting. If in doubt, do not pull the jailed sidebranch guidewire forcefully because the wire may fracture or it can damage the stent as shown in our case. Most reported cases of entrapped wires involved treatment of bifurcation lesions.