
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-050
Presenter
A.A. Sg. Mas Meiswaryasti Putra
Authors
A.A. Sg. Mas Meiswaryasti Putra1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Doni Firman1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1,
View Study Report
TCTAP C-050
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
Left Main DK Crush Stenting in CHIP PCI
A.A. Sg. Mas Meiswaryasti Putra1, Arwin Saleh Mangkuanom1, Amir Aziz Alkatiri1, Doni Firman1
National Cardiovascular Center Harapan Kita, Indonesia1,
Clinical Information
Patient initials or Identifier Number
HO
Relevant Clinical History and Physical Exam
A 69 years old male with a chief complaint of dyspnea on effort since the last 3 months, he also felt angina mostly during moderate activity. He had a history of STEMI anterior without revascularization 4 months earlier in July 2020. His risk factors were hypertension and ex-smoker. His physical examination was unremarkable.
Relevant Test Results Prior to Catheterization
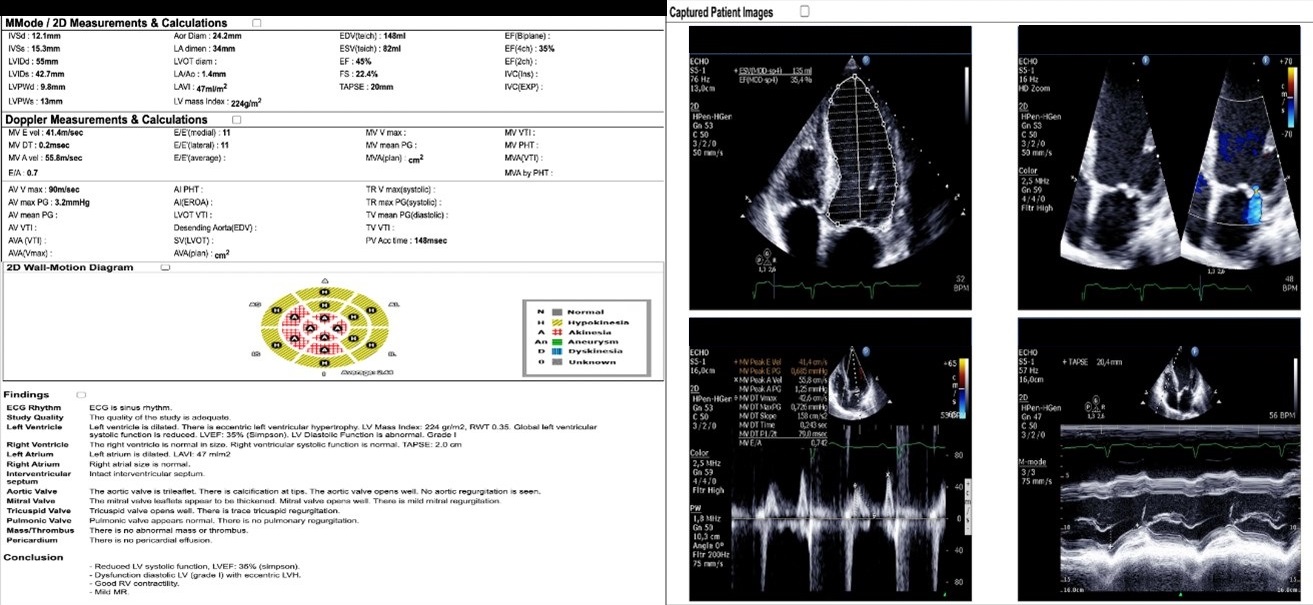
ECG showed sinus bradycardia with heart ra59x/mins, Q wave at infero-anteroseptal. Persistent ST elevation at V4-V5.Echocardiography revealed reduced LV systolic function with EF 34%, hypo-kinetic at mid-basal anteroseptal, apico lateral.Diagnostic CAG showed 3VD with LMS + CTO LAD ( SYNTAX SCORE 51), turned down by surgeon due to not suitable for graft.
 202011111441105704.mov
202011111441105704.mov
Relevant Catheterization Findings
LM: Severe calcification at distal, diffuse stenotic at osteal-distal with maximum stenosis 70-80%, LAD: Severe calcification at proximal; CTO at proximal, distal had flow from contralateral (Rentrop 3), LCx: Dominan, moderate calcification at proximal, subtotal stenosis at osteal, RCA: small calibre, diffuse stenosis 40-50% at ostial-proximal.
Coro_2020_CTO_1_1.mp4
Coro_2020_CTO_4_4.mp4
Coro_2020_CTO_5_5.mp4
Interventional Management
Procedural Step
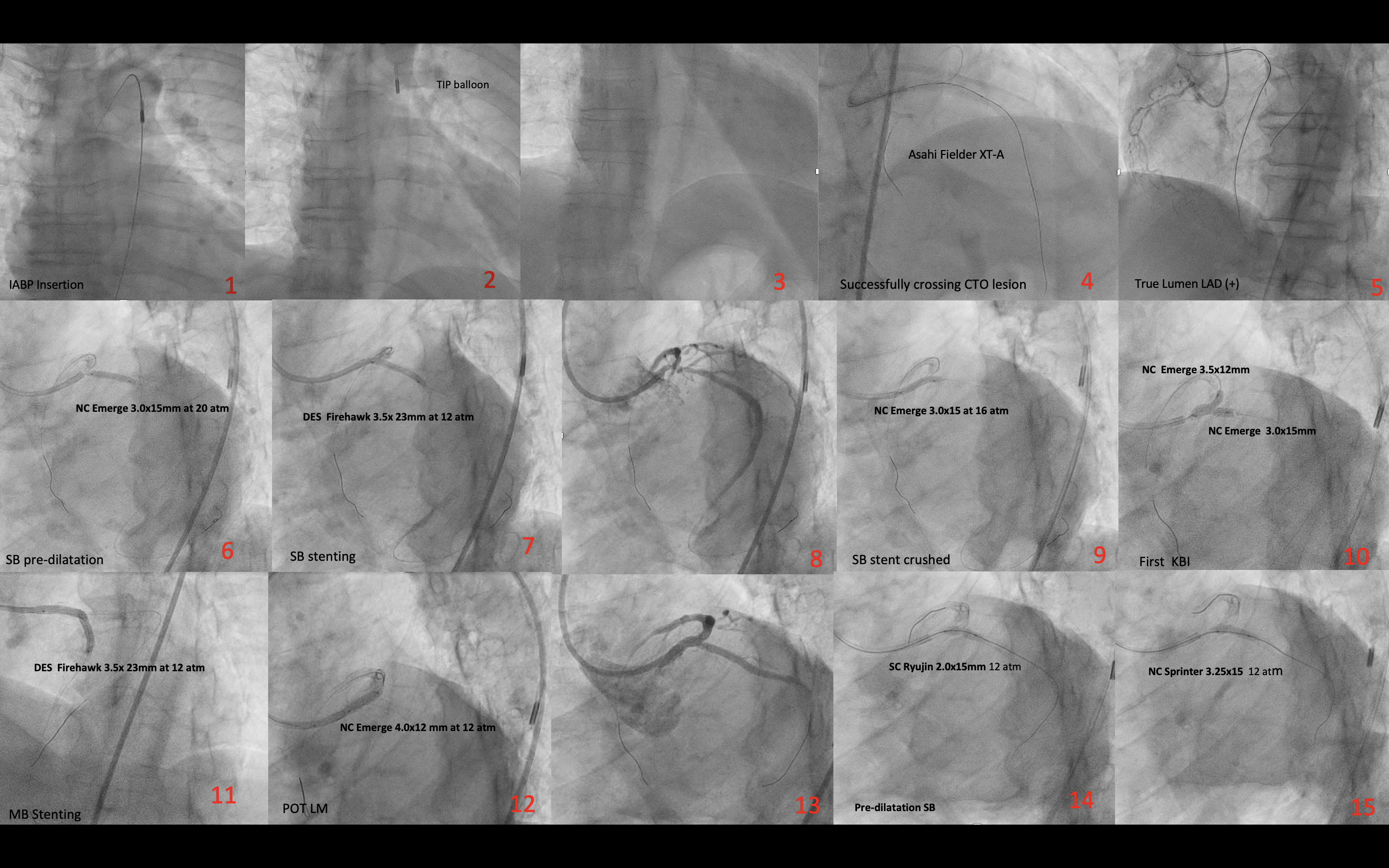
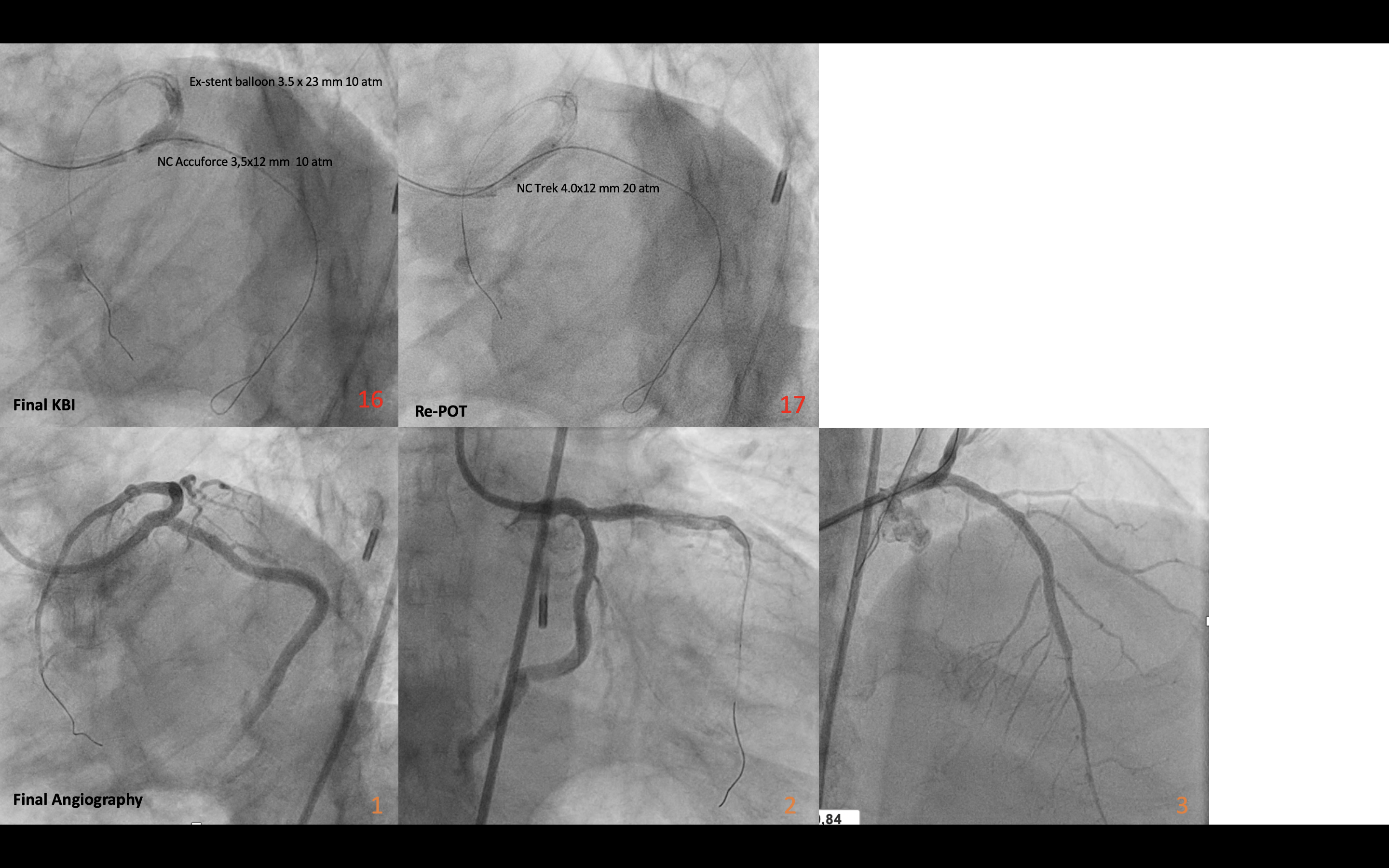
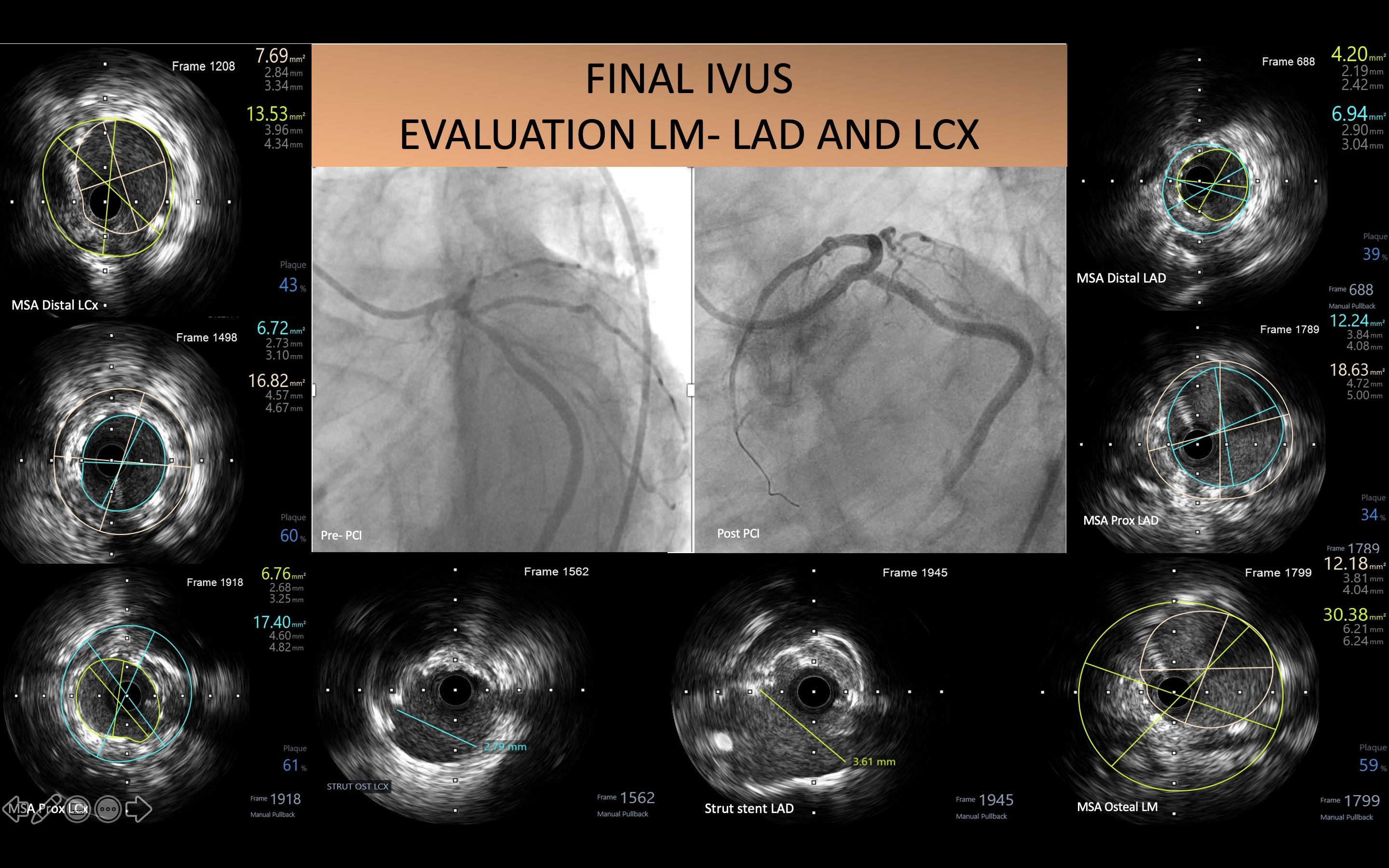
After successful IABP insertion, we planned for PCI CTO LAD with antegrade approach. We crossed the CTO lesion with Fielder XT-A. Pre-dilatation gradually upsized with SC balloon 1.25/20 mm, 2.0/20 mm and 2.5/20 mm. DES Promus Premier 2.5/28 mm was implanted at 11 atm at distal-proximal LAD. Then we continued with LM bifurcation stenting using DK Crush technique. LCx pre-dilatation with SC balloon 2.5/20 mm and NC 3.5/15 mm. DES Firehawk 3.5x23 mm was implanted at 11 atm at proximal LCx with slightly protruding to LM. Crushing the stent was done with NC 3.0/15 mm at 16 atm. Successfully re-crossing wire at proximal strut stent LCx. First KBI was done with NC 3.5/12 mm (LM-LAD) and NC 3.0x15 mm (LM-LCx) at 8 atm. LM-LAD stenting with DES Firehawk 3.5x38 mm at 16 atm at proximal LAD-osteal LM overlapping with the first DES. POT LM was done with NC 4.0/12 atm at 12 atm. Re-crossing wire at proximal strut stent LCx then delivery device with balloon anchoring technique using SC 2.0/20 mm at 6 atm at LAD. Additional post dilatation LCx was needed, gradually upsized with SC 1.25/15 mm, 2.0/15 mm and NC 3.25x15 mm. Final KBI was done with NC 3.5/12 mm (LM-LCx) and stent balloon 3.5/23 mm (LM-LAD) at 10 atm. Re-POT LM with NC 4.0/12 mm at 20 atm. IVUS evaluation showed well-expanded and well-apposed of all stents and no edge dissection was seen. Final angiography showed TIMI 3 flow with good result. One-week clinical follow-up revealed no more chest pain and shortness of breath.
Case Summary
This patient had a severe coronary artery disease and been turned down for surgery revascularization, so high-risk PCI procedure with IABP support was commenced. DK crushed technique was chosen with IVUS guidance due to good outcome from the latest trials for this technique. This CHIP procedure provides a satisfactory result with favorable clinical outcome.