
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-041
Presenter
Tsuda Takuma
Authors
Tsuda Takuma1
Affiliation
Nagoya Ekisaikai Hospital, Japan1,
View Study Report
TCTAP C-041
CORONARY - Chronic Total Occlusion
How Do You Manage It?
Tsuda Takuma1
Nagoya Ekisaikai Hospital, Japan1,
Clinical Information
Patient initials or Identifier Number
N.T.
Relevant Clinical History and Physical Exam
Diagnosis: APPrior intervention: May/2016 emPCI to #6 due to ant-AMI(#6 100%→Xience Alpine4.0/18).
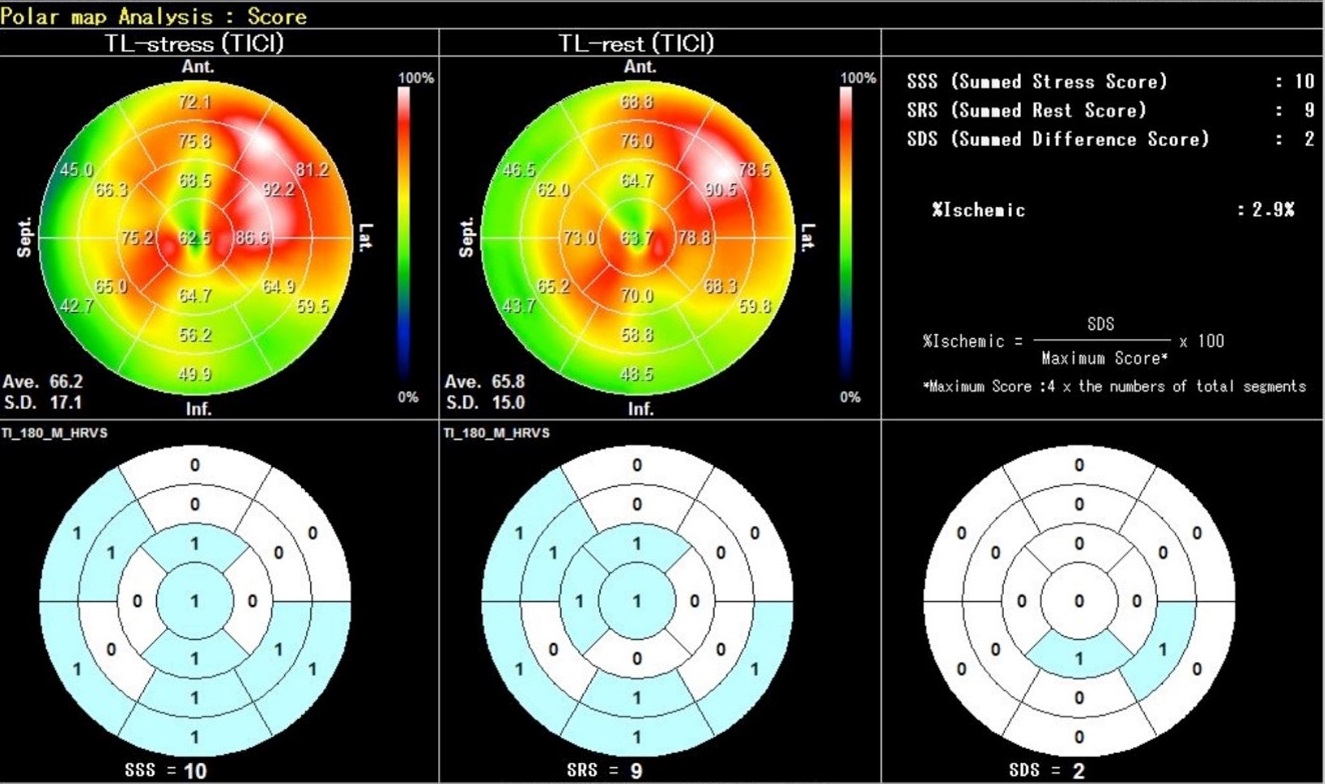
Relevant Test Results Prior to Catheterization
Echocardiography showed EF 43%, ant/inf hypokinesis.CTCA showed long RCA-CTO over 100mm.


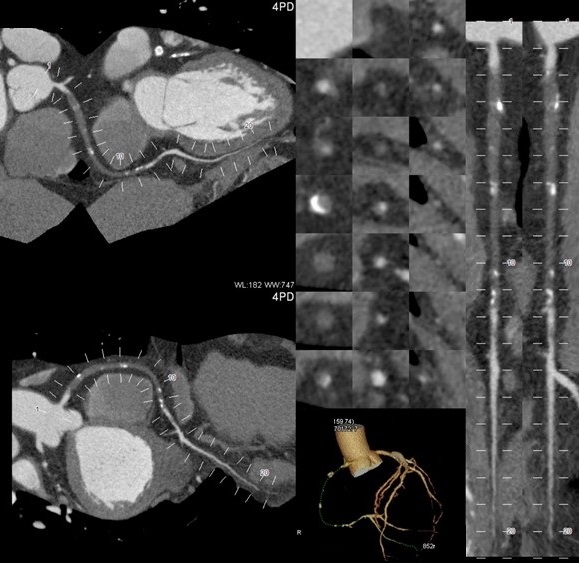
Relevant Catheterization Findings
CAG showed CTO in proximal RCA. Characteristics of CTO entry was stumped, and CTO distal exit was bifurcation of #4-PD and #4-PL.
 RCA-1.mov
RCA-1.mov
LCA-1.mov
LCA-2.mov
Interventional Management
Procedural Step
1. 1st retrograde approach: Sion with Corsair could pass 1st septal
PCI1.mp4
PCI2.mp4
PCI3.mp4
Case Summary
This is the case of RCA CTO with some debatable and educational discussion. In particular, IVUS guided wiring, the way of retrograde set up remained difficult and unclear point during CTO procedure. Here we all learn and share tips for overcoming tough CTO case.