
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-030
Presenter
Marshell Luntungan
Authors
Marshell Luntungan1, Dafsah Arifa Juzar2, Doni Firman2, Daniel Parningotan Tobing2, Amir Aziz Alkatiri2, , Fahmi Shahab2
Affiliation
Prof. Dr. R.D. Kandou Manado General Hospital, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
View Study Report
TCTAP C-030
CORONARY - Bifurcation/Left Main Diseases and Intervention
Left Main Coronary Spasm: Should We Stent?
Marshell Luntungan1, Dafsah Arifa Juzar2, Doni Firman2, Daniel Parningotan Tobing2, Amir Aziz Alkatiri2, , Fahmi Shahab2
Prof. Dr. R.D. Kandou Manado General Hospital, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
Clinical Information
Patient initials or Identifier Number
AK
Relevant Clinical History and Physical Exam
54-year-old male planned to undergo coronary angiography due to chest pain dan shortness of breath especially during moderate activity. Recently he experienced unstable angina. His risk factors are diabetes mellitus and ex-smoker. His physical examination was unremarkable.
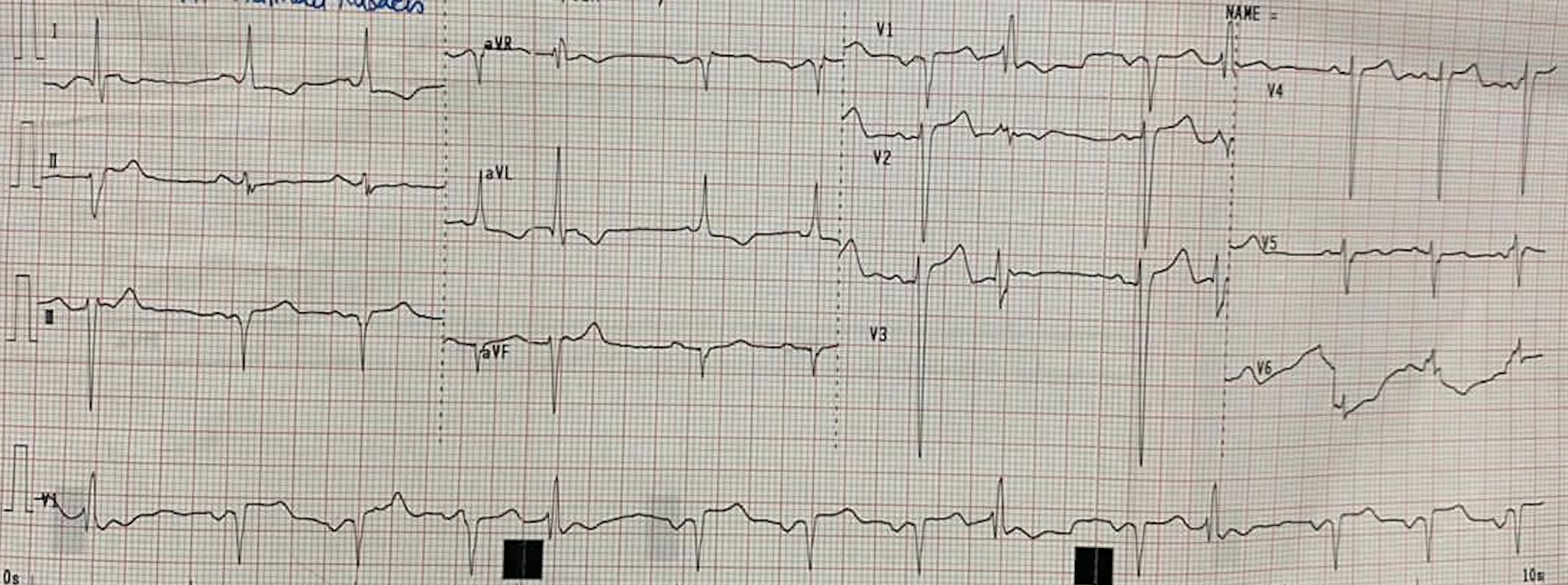
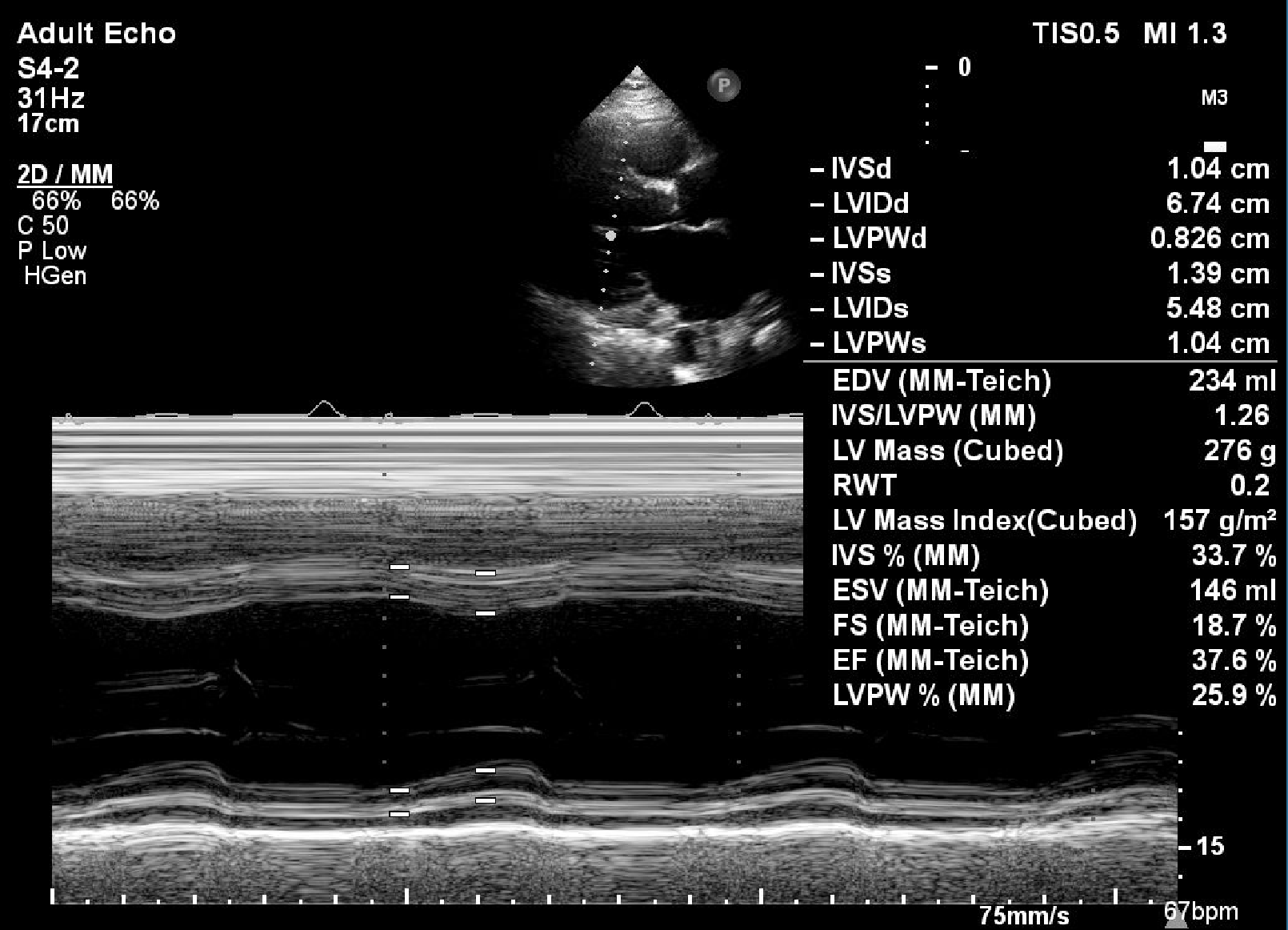
Relevant Test Results Prior to Catheterization
Blood test showed eGFR 57 with HbA1c 5.4%, LDL 77 mg/dL and NTproBNP 298102D echo revealed reduced LV systolic function with EF 36% and akinetic at inferoseptal, apical inferior, mid inferolateral. Eccentric LVH with mild MR.
Relevant Catheterization Findings
Left Main: Critical LM stenosisLAD: Chronic total occlusion after D1, no distal vessel flowLCX: Proximal subtotal occlusionRCA: 80% proximal stenosis, 70-80% distal stenosis
 LCA.mov
LCA.mov
LCA 2.mov
RCA.mov
Interventional Management
Procedural Step
Soon after coronary angiography, the patient complaint severe shortness of breath, diaphoresis and cold extremity. Later on the patient was diagnosed with acute lung edema due to ADHF and cardiogenic shock and was admitted to the CICU. During CICU care for 14 days, despite optimal anti-ischemic the patient still has chest pain and turned down by surgeon for CABG, so our CICU team decided to undergo PCI the next day with IABP as backup.
Procedure:Using JL 4/7F GC, double wiring with floppy wire to LAD and LCx. Wire escalation with Fielder XT-A and GAIA 2 with microcatheter Finecross. During the procedure, the patient complained severe pain on both legs, while on angiography findings showed LM-LAD vessel severely spasm and agian began develop chest pain. Patient was given fentanyl 100mcg IV and IC nitroglycerine 300mcg, but the symptoms and lesion spasm still didn't resolved. We decided to do ballooning of the LM-LAD using Ryujin balloon 3.0x20mm 8atm, continue with PCI with DES Ultimaster 3.5x24mm in LM-LAD and POT with NC balloon 4.0 x 8mm 14atm at the LM. LAD CTO lesion was abandoned and plan for optimal medical therapy. After the procedure, the chest pain was resolved and the patient was discharged 3 days after the PCI.
Screen Recording 2020-11-13 at 08.59.32.mov
Procedure:Using JL 4/7F GC, double wiring with floppy wire to LAD and LCx. Wire escalation with Fielder XT-A and GAIA 2 with microcatheter Finecross. During the procedure, the patient complained severe pain on both legs, while on angiography findings showed LM-LAD vessel severely spasm and agian began develop chest pain. Patient was given fentanyl 100mcg IV and IC nitroglycerine 300mcg, but the symptoms and lesion spasm still didn't resolved. We decided to do ballooning of the LM-LAD using Ryujin balloon 3.0x20mm 8atm, continue with PCI with DES Ultimaster 3.5x24mm in LM-LAD and POT with NC balloon 4.0 x 8mm 14atm at the LM. LAD CTO lesion was abandoned and plan for optimal medical therapy. After the procedure, the chest pain was resolved and the patient was discharged 3 days after the PCI.
Case Summary
Vasospasm of the left main artery may be spontaneous due to inherent endothelial dysfunction or iatrogenic. Short acting nitroglycerine is usually effective in aborting the “attack”. In some cases, PCI may represent an adjunct in the management of focal CAS, although currently medical therapy remains the standard initial approach. In this case, the left main vasospasm didn't resolve with optimal anti-ischemic and even intracoronary nitroglycerine. Due to severe chest pain and hemodynamically unstable, we decided to undergo PCI on the LM-LAD.