
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-014
Presenter
Safir Sungkar
Authors
Safir Sungkar1, Amir Aziz Alkatiri2, Nanda Iryuza2, , Doni Firman2
Affiliation
Dr. Kariadi General Hospital, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
View Study Report
TCTAP C-014
CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS)
Spontaneous Coronary Artery Dissection Complicating ST Elevation Myocardial Infarction in Young Women: To Stent or Not To Stent
Safir Sungkar1, Amir Aziz Alkatiri2, Nanda Iryuza2, , Doni Firman2
Dr. Kariadi General Hospital, Indonesia1, National Cardiovascular Center Harapan Kita, Indonesia2,
Clinical Information
Patient initials or Identifier Number
Mrs. ET
Relevant Clinical History and Physical Exam
A 36-year-old woman, referred to our hospital after fibrinolytic therapy due to anterior MI 2 weeks ago. She had recurrent chest pain. No shortness of breath or palpitation. She had no history of traditional atherosclerotic risk factors. History of preeclampsia 1 year ago. Blood pressure was 120/70 mmHg, HR: 75 bpm, no abnormalities on physical exam.
Relevant Test Results Prior to Catheterization
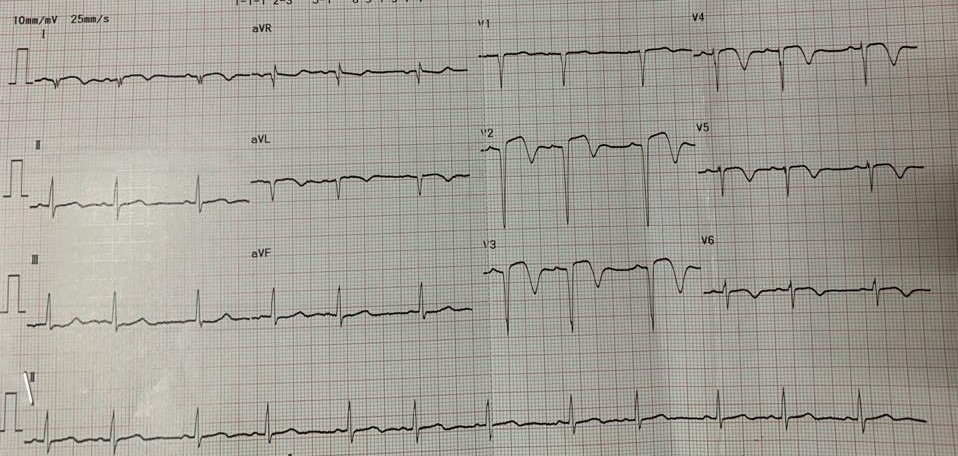
Electrocardiogram showed pathological Q wave and biphasic T wave at precordial leads. Cardiac troponin was elevated and echocardiography revealed hypokinesia at anterior segment and preserved systolic function (LVEF 53%).
 Echo-short axis.mp4
Echo-short axis.mp4
Echo-4ch.mp4
Relevant Catheterization Findings
Coronary angiography (CAG) revealed occlusion at the mid-segment of the LAD with contrast staining at proximal with haziness appearance, while the RCA and LCx were normal.
CAG cra view.mp4
CAG caudal view.mp4
CAG RCA.mp4
Interventional Management
Procedural Step
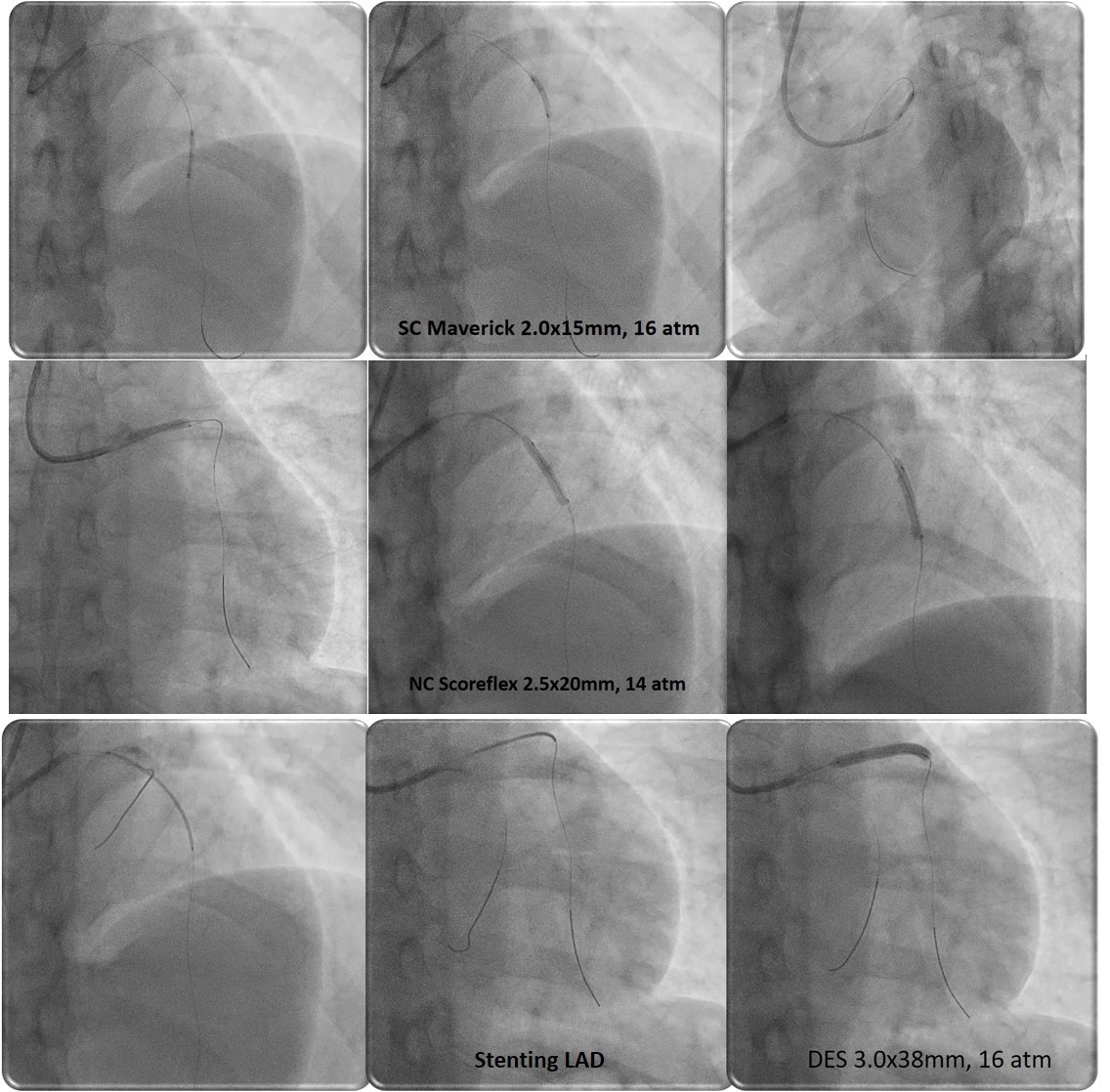
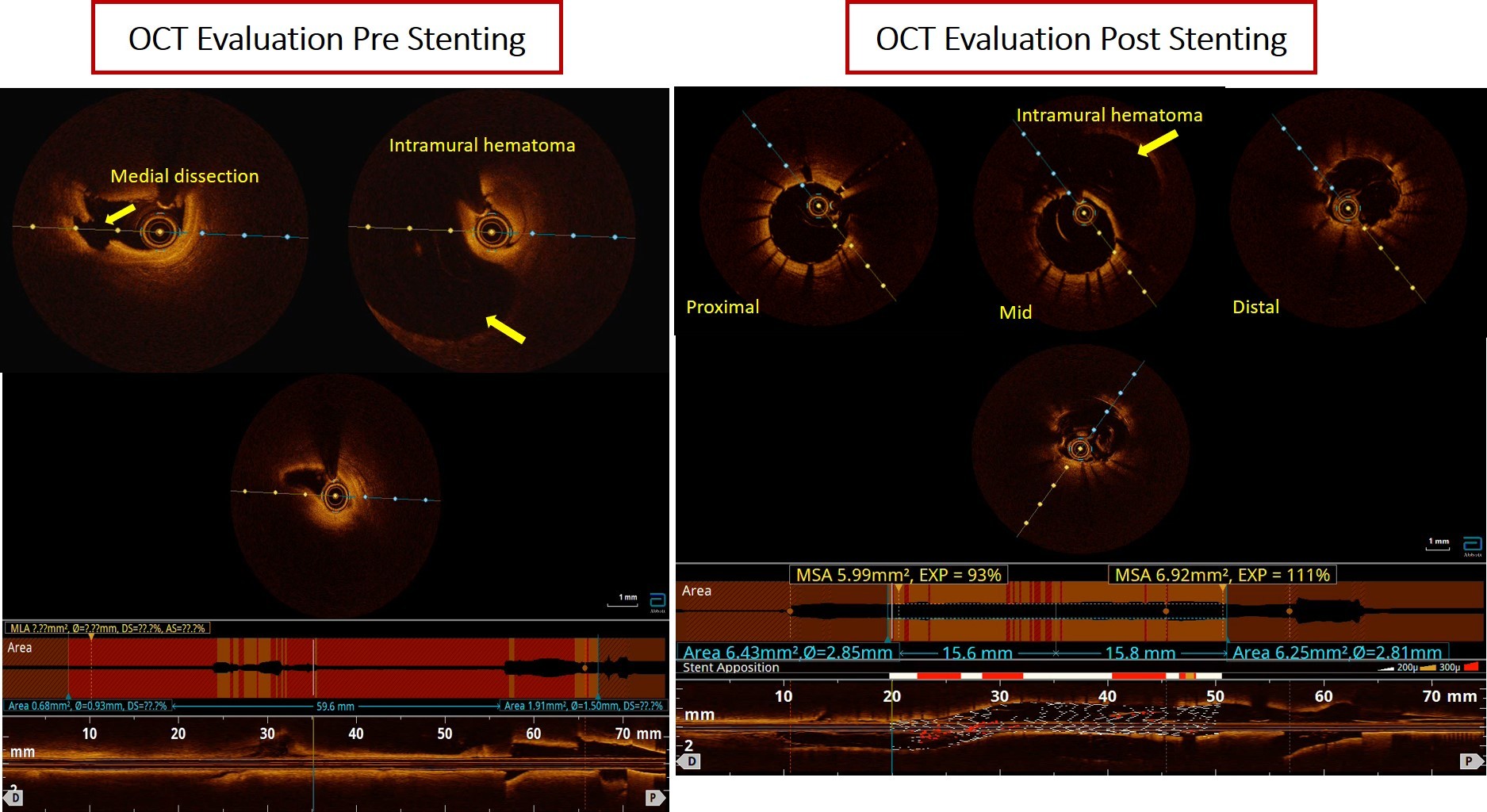
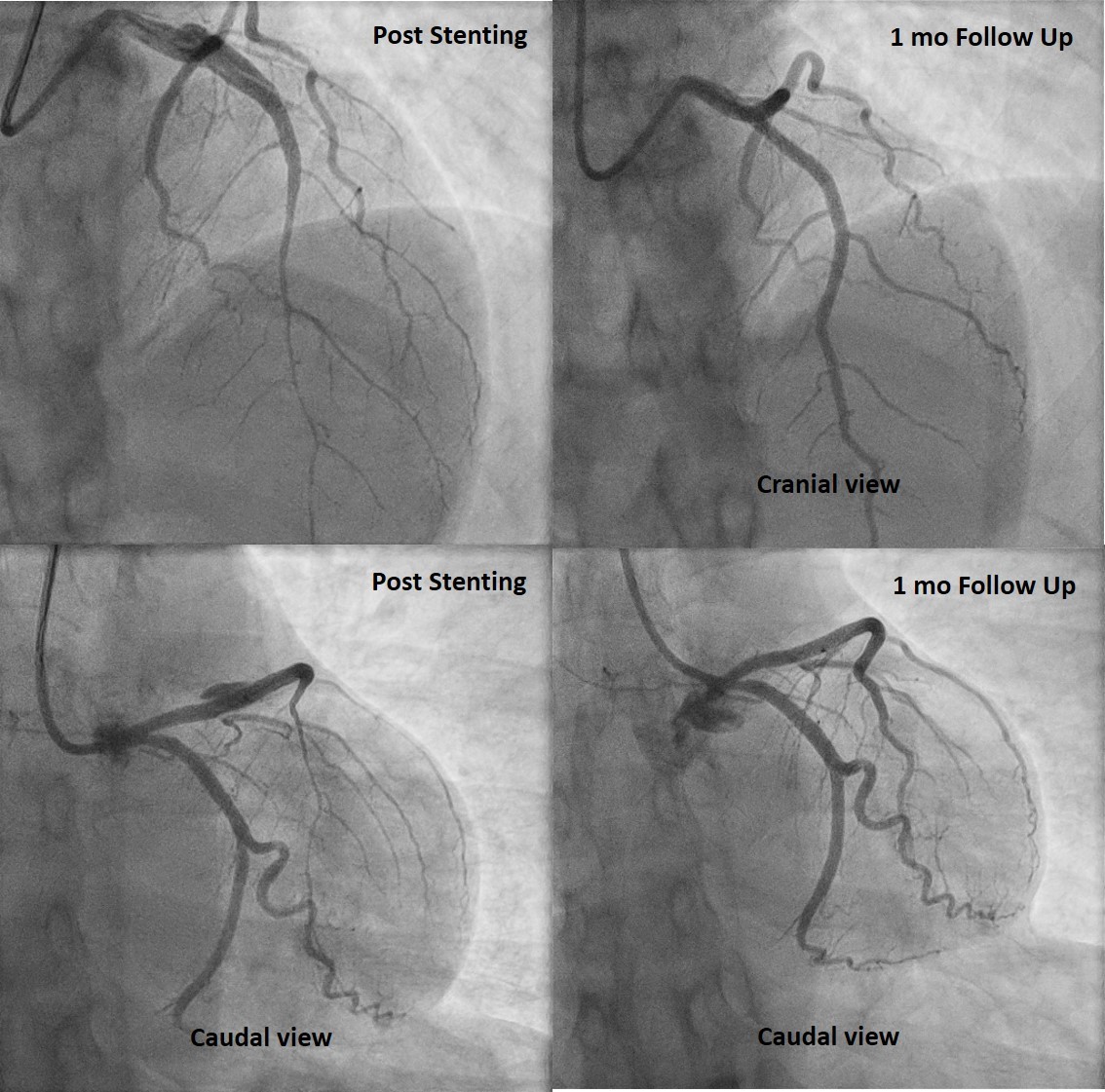
We then proceeded with percutaneous coronary intervention (PCI) of the LAD using GC 3.5/6F. Floppy wire was inserted to distal LAD with microcatheter support, multiple predilatation with SC balloon 2.5 x 20 mm. OCT revealed intramural hematoma 2.5 x 30 mm causing compromise of the true lumen and medial dissection at proximal LAD. Then predilation with NC scoring balloon 2.5 x 20 mm. Stenting DES 3.0 x 38 mm at proximal-mid LAD. Angiographic evaluation showed TIMI 3 flow, no residual stenosis, residual hematoma at proximal LAD. OCT evaluation revealed well apposed and well expanded stent with MSA 6.9 mm2, expansion rate 111%, hematoma and disscetion was covered by stent. At 1 month follow up, coronary angiography revealed complete resolution of SCAD and she had no symptom.
Case Summary
SCAD is infrequent and often missed diagnosis among patients presenting with acute coronary syndrome. In cases where revascularisation is necessary, PCI is generally preferred over CABG if technically feasible. Due to limitation of coronary angiography, OCT provides detailed morphology of the lumen coronary artery including entry tear, intimomedial flap, double-lumenmorphology, intramural hematoma, and associated thrombus and may increase the diagnostic yield as well as guided treatment strategy.