
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-048
Presenter
Michael N. Gergis
Authors
Michael N. Gergis1
Affiliation
Aswan Heart Center (Magdi Yacoub Foundation), Egypt1,
View Study Report
TCTAP C-048
CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP)
CHIP NSTEMI; When Complexity Turns Fruitful at 40 Days
Michael N. Gergis1
Aswan Heart Center (Magdi Yacoub Foundation), Egypt1,
Clinical Information
Patient initials or Identifier Number
Z. A.
Relevant Clinical History and Physical Exam
- 65 years lady, DM, HTN
Relevant Test Results Prior to Catheterization
Echo: severely impaired LVEF = 20% with moderate MR
 pre 1.wmv
pre 1.wmv
pre 2.wmv
Relevant Catheterization Findings
Left main ostial and distal severe stenosis (Medina 1-1-1)LAD: shows tight ostial calcific stenosis followed by mid segment long severe stenosisLCX: retroflexed origin, ostial severe stenosis at the origin of 1st OM branch. The LCX shows proximal long significant stenosisRCA: CTO at the ostium with faint TIMI I and retrograde filling via contralateral septal collateralsHeart team was urgently held and she was turned down by surgeons due to frailty and severely impaired LVEF
pre 2..wmv
pre 3.wmv
pre 4.wmv
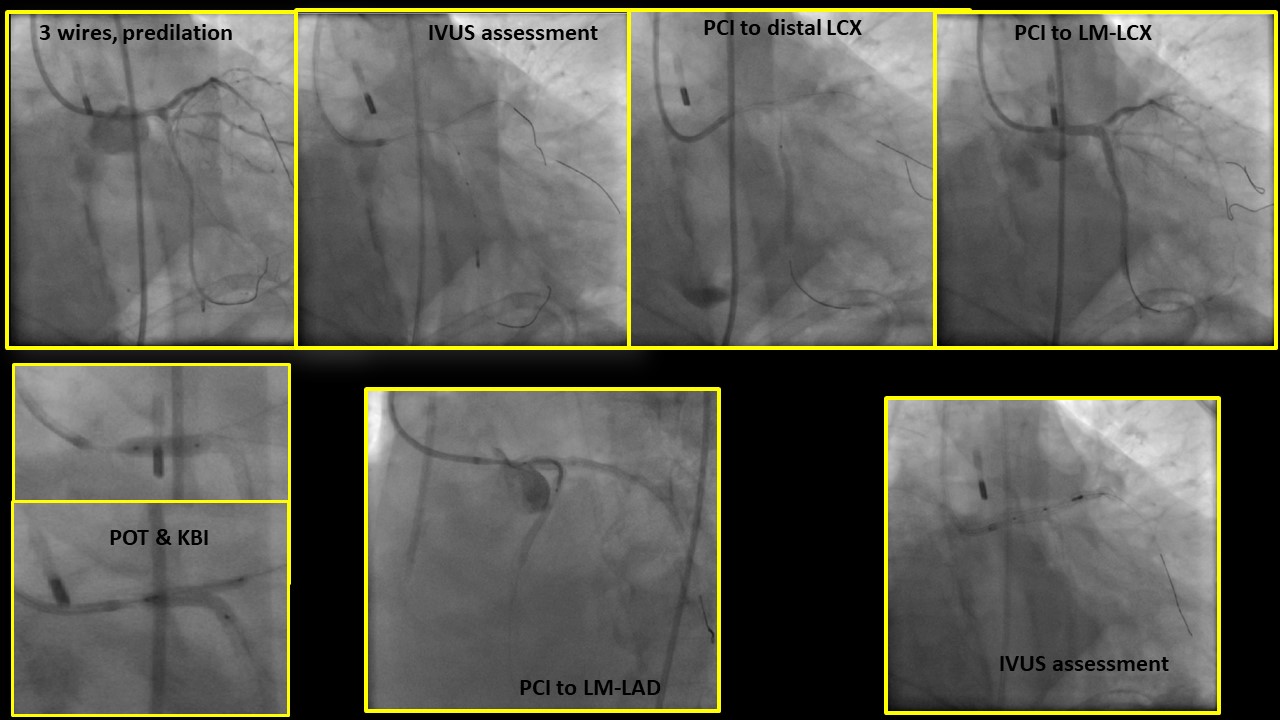
Interventional Management
Procedural Step
> IABP was inserted
post 2.wmv
post echo.wmv
Case Summary
CHIP is not uncommon in daily practice.