
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-026
Presenter
Hosein Alavi
Authors
Seyedhossein Alavi1
Affiliation
Namazi, Iran1,
View Study Report
TCTAP C-026
CORONARY - Bifurcation/Left Main Diseases and Intervention
Double Bifurcation Percutaneous Coronary Intervention in Acute Coronary Syndrome
Seyedhossein Alavi1
Namazi, Iran1,
Clinical Information
Patient initials or Identifier Number
295468
Relevant Clinical History and Physical Exam
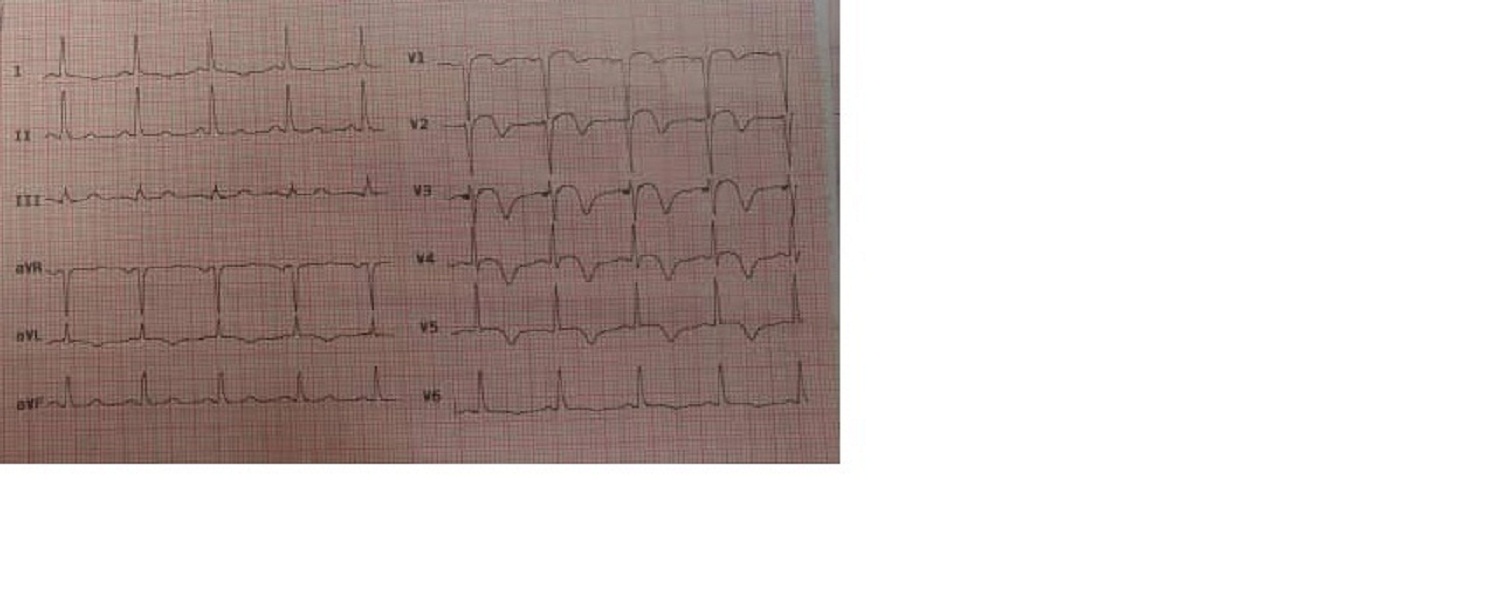
The patient was a 50-year-old gentleman with no prior history of coronary artery disease. He was admitted to the hospital after a new onset of chest pain. Physical examination did not show any significant findings. ST segment elevation and T-wave inversion in anterior leads were detected in the electrocardiogram. He received loading doses of aspirin and clopidogrel and was referred to cardiac catheterization laboratory for primary percutaneous intervention (PCI).
Relevant Test Results Prior to Catheterization
| White blood cells | 7.2 (×103/mcl) | |
| Hemoglobin | 13.1 (gm/dl) | |
| Platelets | 253 (×103/mcl) | |
| Lymphocytes | 0.5 (×10 3/mcl) | 0.9–3.2 (×103/mcl) |
| Sodium | 132 (mmol/L) | 135–145 (mmol/L) |
| Potassium | 5.1 (mmol/L) | |
| Creatinine | 0.90 (mg/dl) | |
| Troponin‐T | 3.6 (ng/ml) | < 0.01 (ng/ml) |
Relevant Catheterization Findings
Left Coronary angiogram showed significant stenosis in the mid of left anterior descending artery followed with muscle bridge. The first large diagonal branch had 90% stenosis ostial and proximal portions. The second diagonal branch also had significant narrowing at its origin. Right coronary angiogram was normal.
 Screen Recording 2020-11-14 at 1.16.05 PM.mov
Screen Recording 2020-11-14 at 1.16.05 PM.mov
Screen Recording 2020-11-14 at 1.16.39 PM.mov
Screen Recording 2020-11-14 at 1.17.09 PM.mov
Interventional Management
Procedural Step
After coronary angiogram, LCA was engaged with EBU 7f guiding catheter. Then two guidewires were passed through LAD and second diagonal branch (D2). After pre-dilation, using the double kissing crush technique, D2 was stented and crushed with an NC balloon and after rewiring, first kissing balloon inflation was performed. Afterward, LAD was stented and second kissing balloon inflation, post dilation and POT were done. Next step was saving the large diagonal branch, so its wiring was done and after pre-dilation with the jailed stent balloon technique, two stents were advanced through LAD and first diagonal branch. The diagonal stent was deployed and after deflation, the stent balloon was pulled back a little. Then LAD stent was inflated. After deflation of the LAD stent balloon, Jailed stent balloon of diagonal branch was reinflated and removed, and finally, LAD stent balloon was reinflated again. Afterward, rewiring of D1 was done and eventually post dilation, kissing balloon inflation and POT were done with a nice final result.
first bifurcation.mov
second bifurcation.MOV
final result.MOV
Case Summary
Saving the Coronary side branch is a mandatory step in saving the myocardium, especially if it is a large side branch.In this particular case both diagonal branches supplied a large myocardial territory, and that is why saving it was of great importance.Double kissing crush technique for both bifurcation lesions needed more time.The use of jailed stent balloon technique, in this case, has good short and medium-term results.The jailed stent balloon technique is especially useful in acute coronary syndrome for shortening the procedural time.