TCTAP C-062
CORONARY - Complications
Iatrogenic Retrograde Coronary Aortic Dissection During Coronary Intervention: Rare But Life-threatening
Ramachandran Sathappan1, Tze Ming Chan2, Yew Fung Kwan3, Benjamin Tao Xiung Lim4, Jian-Chen Lim5, Hameeth Shah Abdul Wahid4, Mohd Ruslan Mustapa6, Gurpreet Pal Singh Jugindar Singh4, Hazleena Mohamed Hasnan4, Nor Hanim Mohd Amin4
Hrpb Ipoh, Malaysia1, Columbja Asia petaling Jaya, Malaysia2, Hospital Raja Permaisuri Bainun Ipoh, Malaysia3, Hospital Raja Permaisuri Bainun, Malaysia4, Hospital Serdang, Malaysia5, Sultan Idris Shah Serdang Hospital, Malaysia6,
Clinical Information
Patient initials or Identifier Number
HRPB 524763
Relevant Clinical History and Physical Exam
59-year-old Asian man with underlying hypertension, type 2 diabetes mellitus and Ischemic heart disease. He had a history of Non ST Elevation Myocardial infarction on February 2020. Cardiac catheterization showed 90% stenosis of distal LCx and chronic total occlusion of proximal LAD with good collaterals from RCA. The culprit distal LCx lesion was treated with a drug coated balloon. In view of still symptomatic, he was electively planned for proximal LAD CTO intervention.
Relevant Test Results Prior to Catheterization
Echocardiogram showed ejection fraction of 35% with anteroseptal hypokinesis.
Relevant Catheterization Findings
Catheterization with dual injection was done using Bi- radial approach (right radiac and left distal radial/snuffbox access) to study the CTO lesion. LM was short and smooth, ostial LAD was subtotal followed by proximal CTO with good collaterals from the RCA, distal LCx which was previously treated with a DCB showed 90% stenosis. Proximal LAD CTO segment had a clear tapered proximal cap with the lesion length of <20mm. J-CTO score was 0. RCA was dominant with minor irregularities.
 Catheterization findings.mp4
Catheterization findings.mp4Interventional Management
Procedural Step
Case Summary
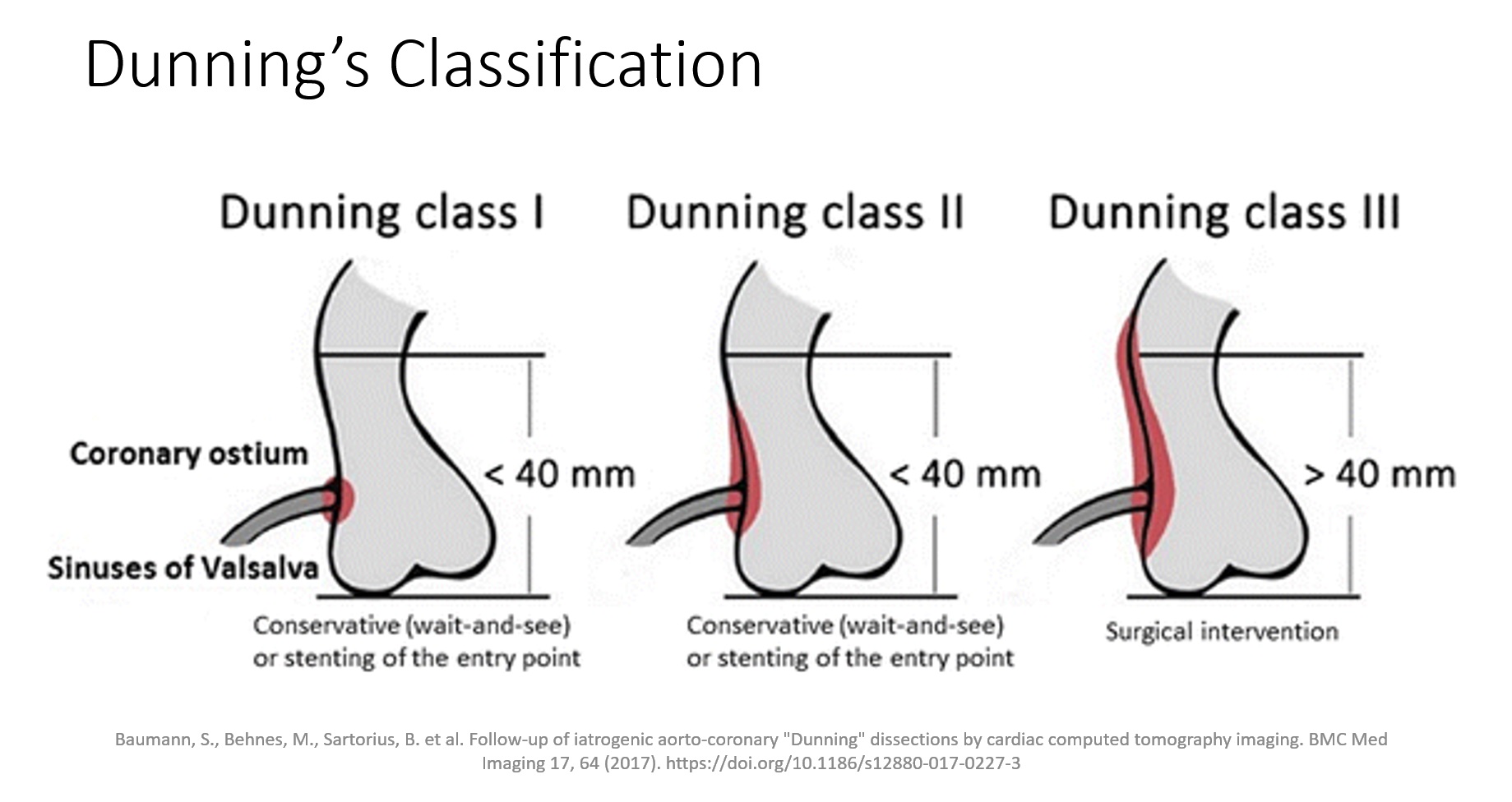
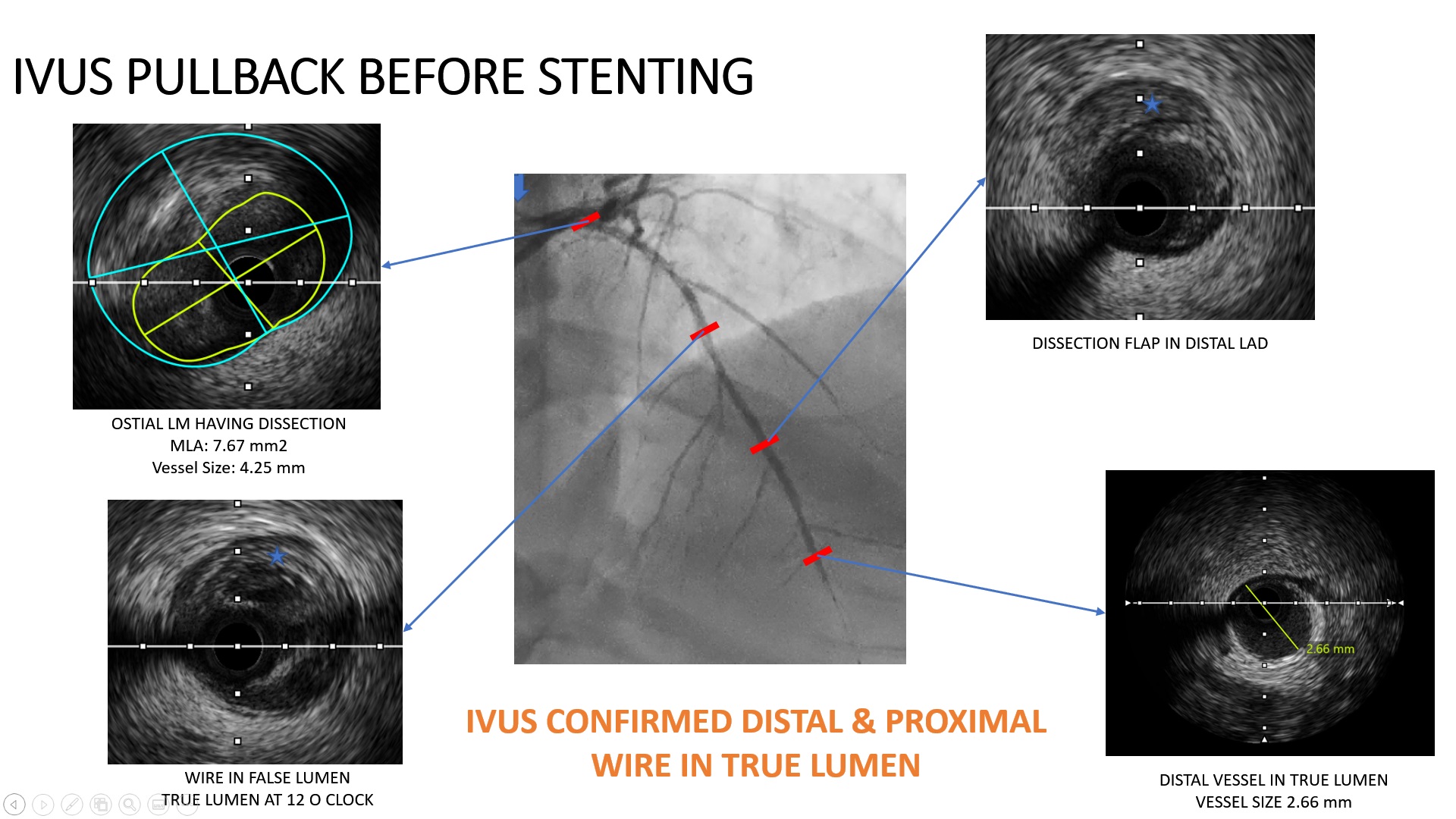
Iatrogenic retrograde coronary aortic dissection is a rare and potentially catastrophic complication mostly originates from catheter-induced trauma, wire induced trauma or balloon inflation, especially to the LMCA. Surgery is the choice of treatment, but in these retrograde dissections ostial stenting is an alternative. T-stenting can be done during emergencies as access to the main branch is maintained throughout the procedure. Steps are fewer which ensures expeditious coverage of both vessels followed by the kissing and proximal optimization. It also allows operators to start with a provisional strategy and convert to T-stenting should the need arise.