
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP C-081
Presenter
Hoong Sheng Loh
Authors
Hoong Sheng Loh1
Affiliation
National Heart Institute, Malaysia1,
View Study Report
TCTAP C-081
CORONARY - Pharmacology/Pharmacotherapy
Big and Stubborn: Persistent Intracoronary Thrombus
Hoong Sheng Loh1
National Heart Institute, Malaysia1,
Clinical Information
Patient initials or Identifier Number
NM
Relevant Clinical History and Physical Exam
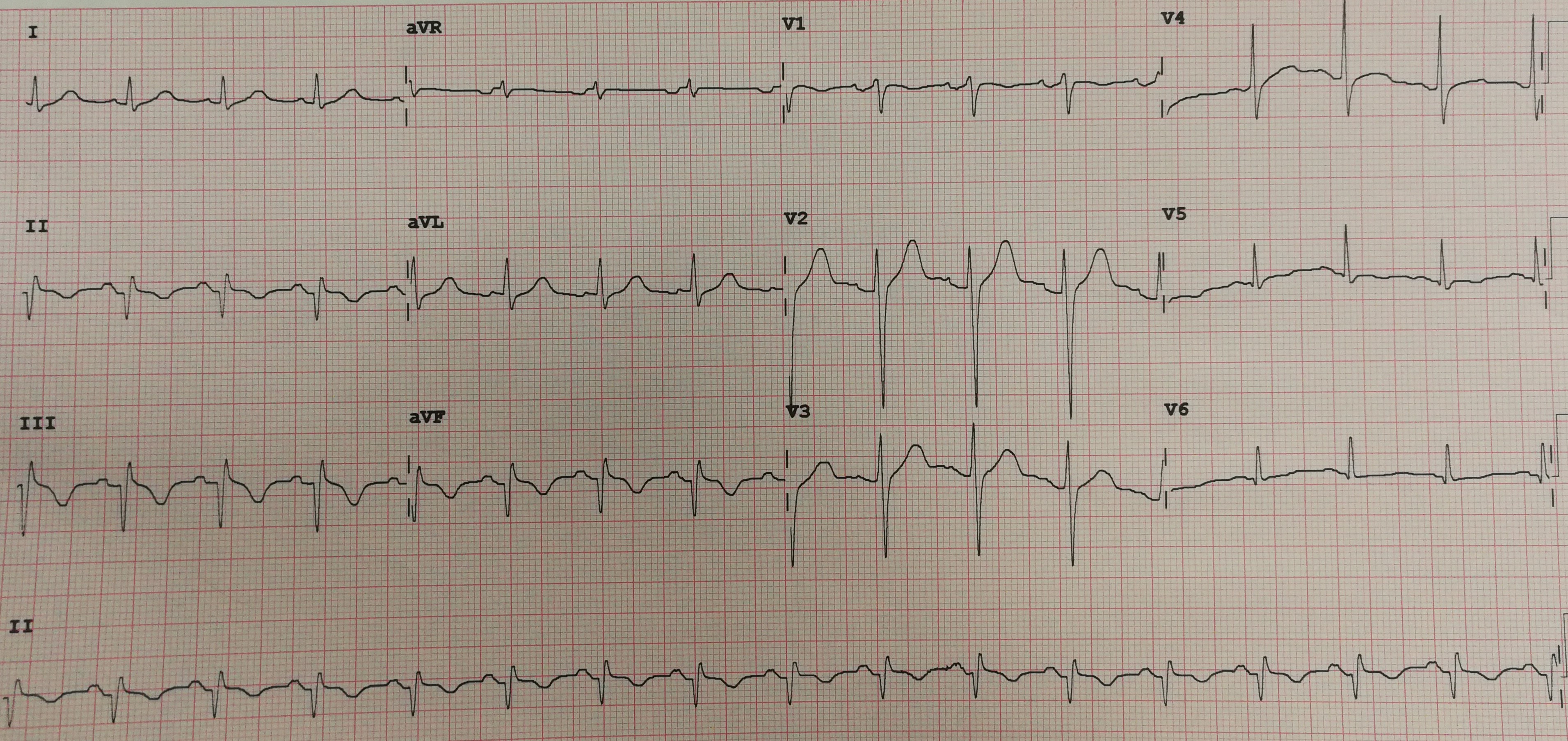
A 56-year-old male, with 40-pack-year of smoking and dyslipidemia, presented to a district hospital after 6 hours of sudden chest pain. He was hemodynamically stable. ECG showed sinus rhythm with ST-segment elevation in inferior leads suggestive of inferior STEMI. Since there was no cardiac catherization facility nearby, he was given oral aspirin with clopidogrel and successfully thrombolysed with IV streptokinase. He was then referred to a cardiac centre for early coronary angiogram.
Relevant Test Results Prior to Catheterization
Repeat ECG at the cardiac centre showed sinus rhythm and complete resolution of ST-segment elevation with T-wave inversions in the inferior leads. Echocardiogram showed left ventricular ejection fraction of 50% with inferior and posterior wall hypokinesia.
Relevant Catheterization Findings
Coronary angiogram performed 1 week later after the acute presentation showed total occlusion (TIMI Thrombus grade 5) from proximal RCA (dominant vessel) with high thrombus burden. The left coronaries were normal.
 RCA-1.avi
RCA-1.avi
LAD-1.avi
LCX-1.avi
Interventional Management
Procedural Step
Thrombus aspiration was attempted with Export Advance catheter and TIMI 2 flow was achieved. In view of persistent high thrombus burden, IV glycoprotein IIb/IIIa inhibitor (Tirofiban) was given for 36 hours with subcutaneous fondaparinux for 5 days. He remained stable without angina. Repeat coronary angiogram showed persistent heavy thrombus burden in the RCA with TIMI 2 flow. Thrombus aspiration was attempted again but failed to achieved satisfactory result for intracoronary imaging or stenting. Mechanical thrombectomy device was not available in our centre. Therefore, it was decided that the patient needed a longer duration of antithrombotic therapy before repeat coronary angioplasty. Patient had a very low bleeding risk score. After a comprehensive discussion, considering the risks and benefits he chose a trial of dual antiplatelet therapy with Rivaroxaban 20mg daily for 1 month. He was not keen for oral vitamin K antagonist or subcutaneous low molecular weight heparin. He returned 1 month later and coronary angiogram showed complete resolution of intracoronary thrombus with moderate lesion in mid RCA. Fraction flow reserve was 0.98 and we decided that stenting was not required. He was discharged with DAPT plus standard guideline-directed medical therapy and remained well during his first year of follow-up.
RCA-post-aspiration.avi
RCA-2nd CAG.avi
RCA-3rd CAG.avi
Case Summary
This case demonstrated a persistent heavy intracoronary thrombus burden in a patient with recent inferior STEMI despite given IV streptokinase, dual oral antiplatelet therapy, IV glycoprotein IIb/IIIa inhibitor, subcutaneous low molecular weight heparin and multiple attempts of thrombus aspiration. Further intracoronary intervention was delayed to allow for longer duration of antithrombotic therapy with DAPT and direct oral anticoagulant (DOAC) till one month, which resulted in complete resolution of intracoronary thrombus and prevented angioplasty of a vessel without significant stenosis. However, further trials or evidence are needed for management of similar cases.