
Lots of interesting abstracts and cases were submitted for TCTAP 2021 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
TCTAP A-040
Presenter
Mahmoud Khalil
Authors
Mahmoud Khalil1, Ahmed Shahin1, Mohamed Abouelasaad1, Ahmed El Shall1, Mohamed Senara1, Ahmed M. Elsharkawy1, Ahmed Mashaly2, Alaa Mohamed Reda1, Amr Elsheikh1, Osama Shoeib1
Affiliation
Tanta University Hospital, Egypt1, Korea University Guro Hospital, Korea (Republic of)2
View Study Report
TCTAP A-040
Peripheral Vascular Disease and Intervention
Common Femoral Artery Anatomy and Relations to Bony Landmarks: A Computed Tomography Angiogram Among Egyptian Population
Mahmoud Khalil1, Ahmed Shahin1, Mohamed Abouelasaad1, Ahmed El Shall1, Mohamed Senara1, Ahmed M. Elsharkawy1, Ahmed Mashaly2, Alaa Mohamed Reda1, Amr Elsheikh1, Osama Shoeib1
Tanta University Hospital, Egypt1, Korea University Guro Hospital, Korea (Republic of)2
Background
Despite the advantages of the radial artery access over the femoral approach, femoral access remains the main access in some interventions that require large sheathes as Trans aortic valve replacement (TAVR). Vascular complications are considered one of the frequent complications to arterial and particularly femoral access, With the wide adoption of the radial access femoral access complications may increase due to lack of expertise and daily practice.
Methods
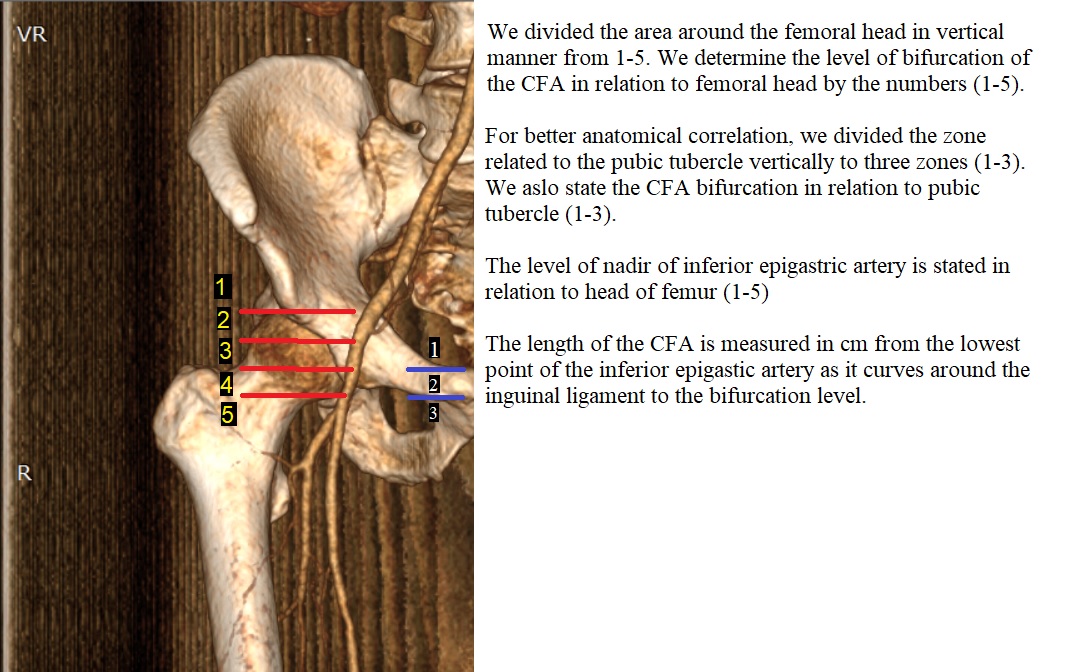
We retrospectively collected all CT peripheral angiograms done in the period from July 2019 to July 2020 that includes femoral artery on both sides. multiplanar reconstruction (MPR) mode is used to determine the start of the common femoral artery (CFA) by the returning point of the inferior epigastric artery and the end is defined by the point of distal bifurcation. Dimensions and length of CFA were measured in the MPR mode on both sides.
Results
414 femoral arteries were reviewed in CT scans. 34 were excluded either due to occluded femoral arteries or due to poor opacification, and 380 were included in the study.
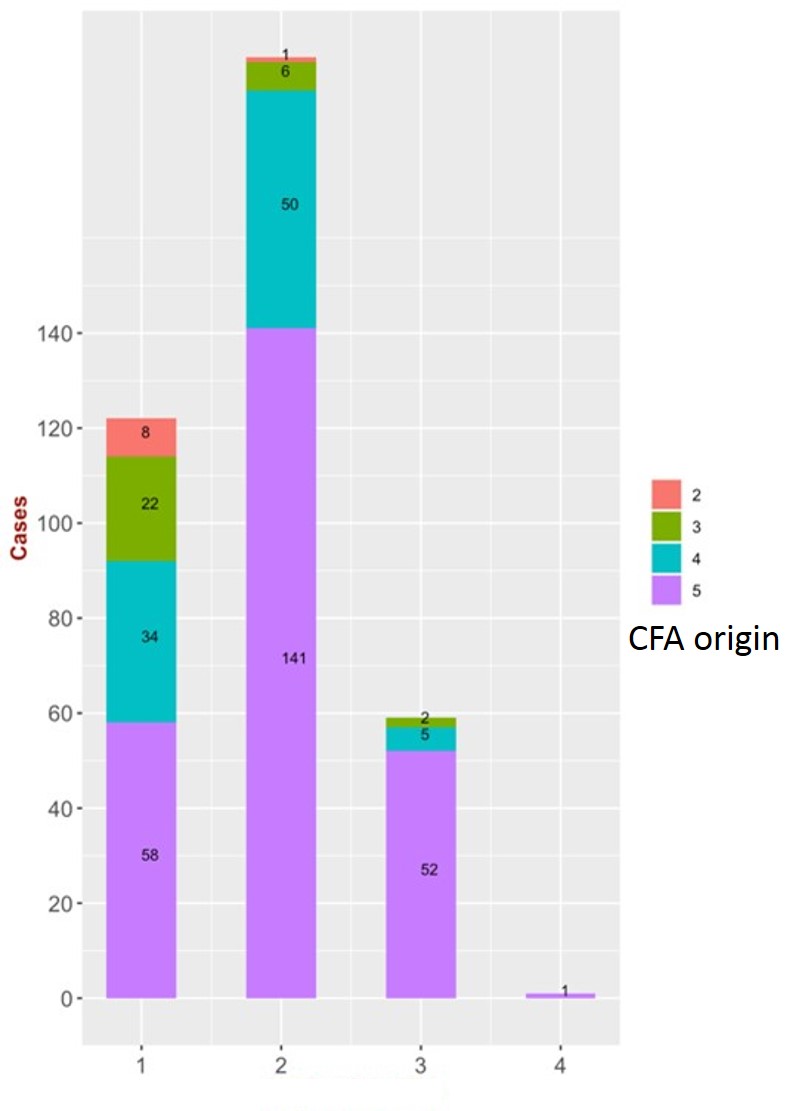
Origin of the common femoral artery:
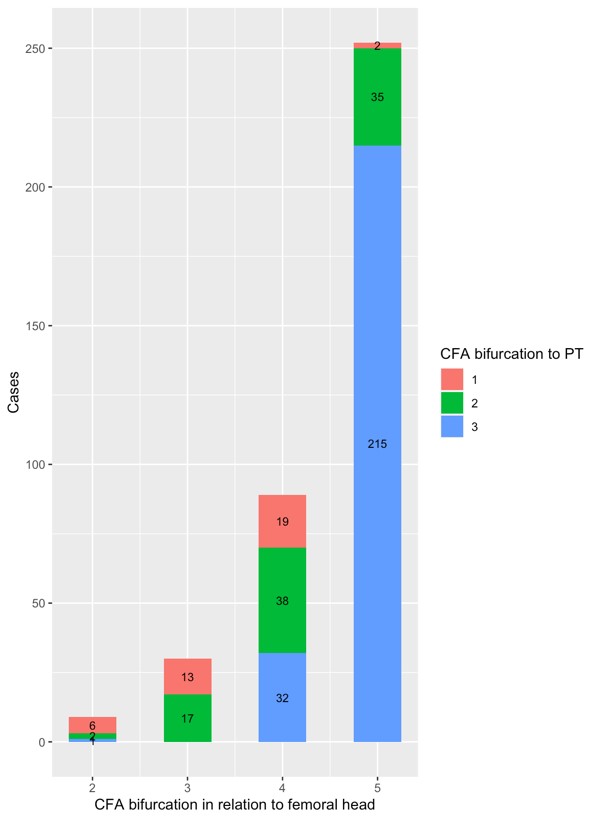
Common femoral artery bifurcation: The bifurcation site was reviewed in relation to both the femoral head and the pubic tubercle. While zone 3 seems to be a safer option than zone 4 in terms of avoiding low puncture, adding the pubic tubercle in consideration -with a puncture in zone 4 or 5 above the pubic tubercle- can increase the probability of avoiding a low puncture (X-squared = 79.859, df = 1, p-value < 2.2e-16).
| Min. | Max. | mean | SD | Gender variation (Anova) | |
| Length (cm) | 0.4 | 11.26 | 4.43 | 1.37 | 0.0197 |
| Min diameter | 1.1 | 14.4 | 7.81 | 1.88 | 0.241 |
| Max diameter | 2.2 | 15.8 | 9.047 | 1.8 | 0.11 |
| Avg diameter | 2.35 | 14.50 | 8.44 | 1.75 | 0.146 |
Origin of the common femoral artery:
| Nadir of IEA | n (380) |
| 1 | 122 (32.1%) |
| 2 | 198 (52.1%) |
| 3 | 59 (15.6%) |
| 4 | 1 (0.26 %) |
Common femoral artery bifurcation: The bifurcation site was reviewed in relation to both the femoral head and the pubic tubercle. While zone 3 seems to be a safer option than zone 4 in terms of avoiding low puncture, adding the pubic tubercle in consideration -with a puncture in zone 4 or 5 above the pubic tubercle- can increase the probability of avoiding a low puncture (X-squared = 79.859, df = 1, p-value < 2.2e-16).
| CFA bifurcation level to the femur head | n = 380 | CFA bifurcation level to the pubic tubercle | n = 380 |
| 1 | 0 | 1 | 40 (10.5%) |
| 2 | 9 (2.4%) | ||
| 3 | 30 (7.9%) | 2 | 92 (24.2) |
| 4 | 89 (23.4%) | 3 | 248 (65.2%) |
| 5 | 252 (66.3%) |
Conclusion
The vascular complication in intervention cardiology still depilating, so blind femoral artery puncture even with experienced operator is not advised. Using imaging guidance can decrease such complications and improve patient's outcome. The availability of ultrasound machines may not be available in all Cath lab especially in countries with low budgets. As the fluoroscope is available so we examined the combination of fixed bony landmarks to guide the femoral artery puncture with such an easy and readily available tool. combining the femoral head and the pubic tubercle can provide more safety during femoral puncture.