
Lots of interesting abstracts and cases were submitted for TCTAP 2025. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge and interact with authors as well as virtual participants by sharing your opinion in the comment section!
TCTAP C-095
Chronic Total Occlusion of Left Anterior Descending Artery: A Case Report of Antegrade Approach With Usage of Dual Lumen Microcatheter With Buddy Wire Support
By Syed Saleh Syed Sheikh, New Rupeng, Muhammad Azlan Aseri, Mohd Aizuddin Mohd Zulastri, Koshi Matsuo, Wan Azman Wan Ahmad, Ahmad Syadi Mahmood Zuhdi, Lee Kee Wei
Presenter
Syed Saleh Syed Sheikh
Authors
Syed Saleh Syed Sheikh1, New Rupeng2, Muhammad Azlan Aseri2, Mohd Aizuddin Mohd Zulastri2, Koshi Matsuo3, Wan Azman Wan Ahmad2, Ahmad Syadi Mahmood Zuhdi2, Lee Kee Wei2
Affiliation
Sultan Ahmad Shah Medical Centre, Malaysia1, University Malaya Medical Centre, Malaysia2, Yao Tokushukai General Hospital, Japan3,
View Study Report
TCTAP C-095
Coronary - Complex PCI - CTO
Chronic Total Occlusion of Left Anterior Descending Artery: A Case Report of Antegrade Approach With Usage of Dual Lumen Microcatheter With Buddy Wire Support
Syed Saleh Syed Sheikh1, New Rupeng2, Muhammad Azlan Aseri2, Mohd Aizuddin Mohd Zulastri2, Koshi Matsuo3, Wan Azman Wan Ahmad2, Ahmad Syadi Mahmood Zuhdi2, Lee Kee Wei2
Sultan Ahmad Shah Medical Centre, Malaysia1, University Malaya Medical Centre, Malaysia2, Yao Tokushukai General Hospital, Japan3,
Clinical Information
Patient initials or Identifier Number
Relevant Clinical History and Physical Exam
Clinical Information
Relevant Test Results Prior to Catheterization
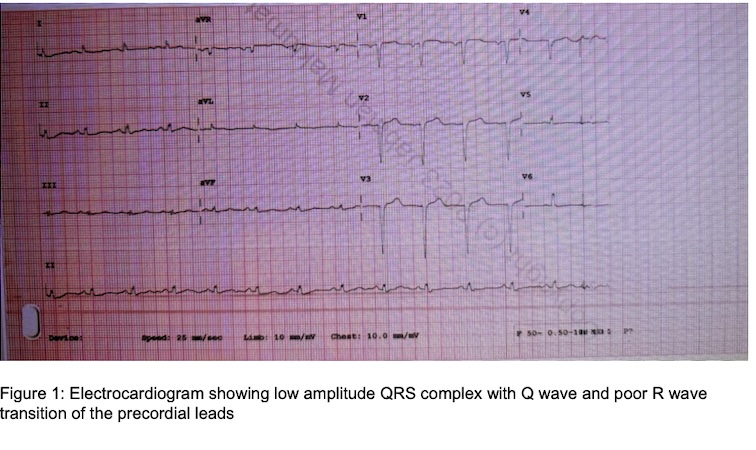
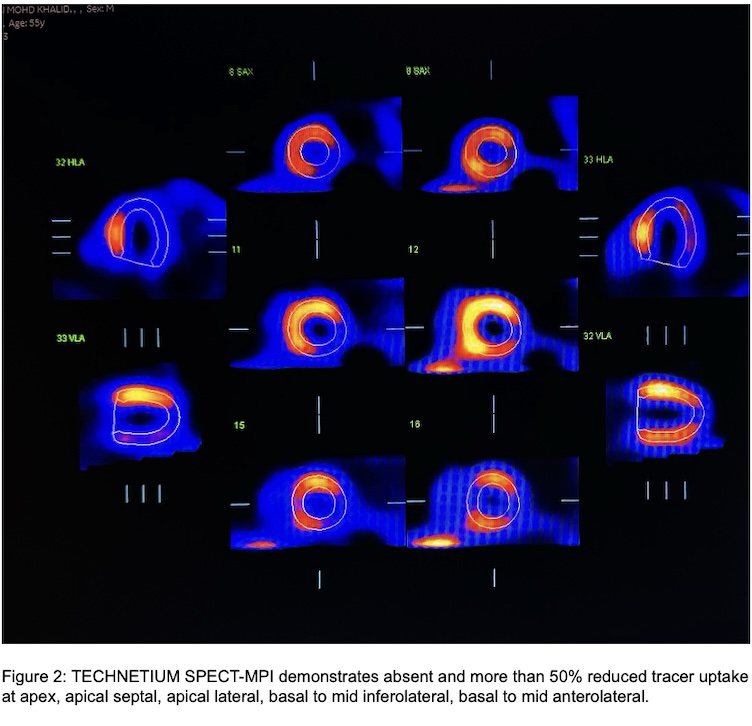
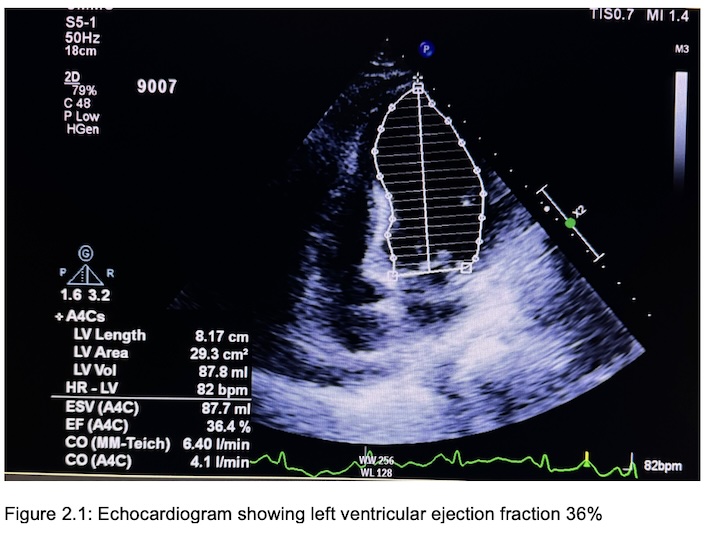
Electrocardiogram demonstrates sinus rhythm with Q wave at V2-V3 and poor R wave transition, while troponin is elevated at 19,000. Echocardiogram shows dilated left ventricle with left ventricular ejection fraction of 36%. 8 left ventricular segments are hypokinetic. Non ST elevation myocardial infarction is diagnosed. Subsequent SPECT myocardial perfusion imaging demonstrates 5 non viable segments of left circumflex territory, and 2 segments of left anterior descending territory
Relevant Catheterization Findings
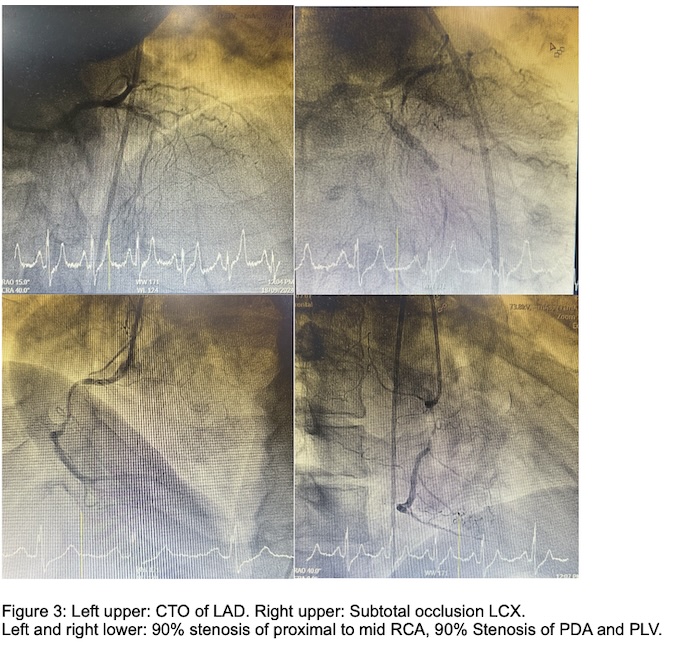
Diagnostic coronary angiogram via the right femoral artery using a 6Fr Judkins Left 4.0 demonstrates a CTO of the proximal LAD and 99% stenosis of the mid-distal LCX. This is followed by a coronary angiogram using Judkins Right 3.5 that demonstrates the presence of 80-90% stenosis of the proximal RCA, 80-90% stenosis of both the PLV and PDA. The distal RCA contributes bridging collaterals to the LAD.
Interventional Management
Procedural Step
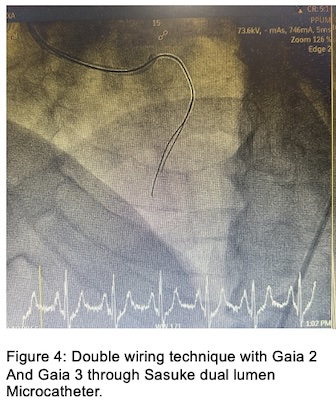
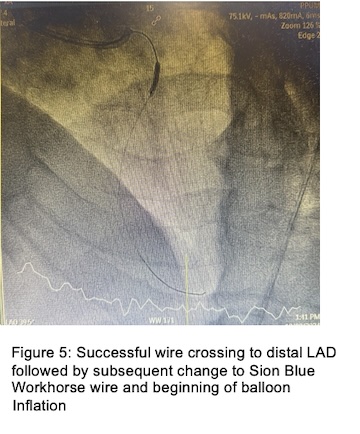
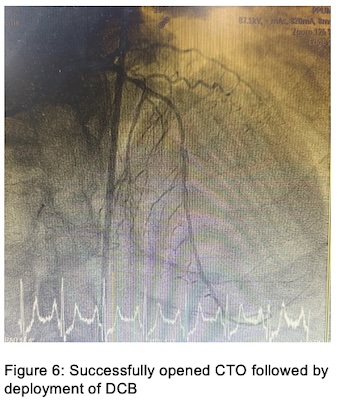
Subsequently, decision was made to intervene the LAD CTO via an antegrade approach via single puncture strategy. Angioplasty began by engaging a 7Fr Judkins Left 4.0 to the left coronary ostium. Wiring was initially performed using a Sion Blue through a Fine Cross microcatheter which was unsuccessful as the wire was only able to tunnel the CTO cap but could not advance further down. As a result, the wire was changed to Gaia Second via trapping ballon technique using Genoss 2.5 x 12 inflated at 12 atm. At this stage, Gaia Third was passed through a Sasuke double lumen catheter acting as a support wire. As a result, Gaia Second was able to be tunneled through the CTO reaching the distal LAD. Angiographic image captured confirmed the location of the wire within the true lumen. Serial predilation was performed using Sapphire 0.85 x 5, followed by Pantera Pro 1.25 x 15 at 14 atm, and finally Sapphire 2.0 x 15. Satisfactory expansion was achieved with a non flow limiting (Type B) dissection. DCB was eventually deployed with Magic Touch 2.25 x 40 at 8 atm for 60 seconds leading to a fully restored main vessel together with its side branches. Subsequent outpatient follow up review revealed improvement of left ventricular ejection fraction to 45%.
Case Summary
This case illustrates the key interventional strategies when dealing with intervention of CTO. Wire crossing through the CTO lesion is crucial since only successful wiring could further permit balloon crossing. Several additional techniques to aid in successful wire crossing include ballon over wire support, microcatheter and stiff wire usage can be implemented. However, extreme caution should be taken when using stiff wires as the risk of subintimal wiring resulting in the creation of false lumen may happen. Finally, avoiding creation of false lumen is the utmost important aspect to pre-empt unwanted subintimal balloon dilation which may result in devastating coronary perforation.